 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
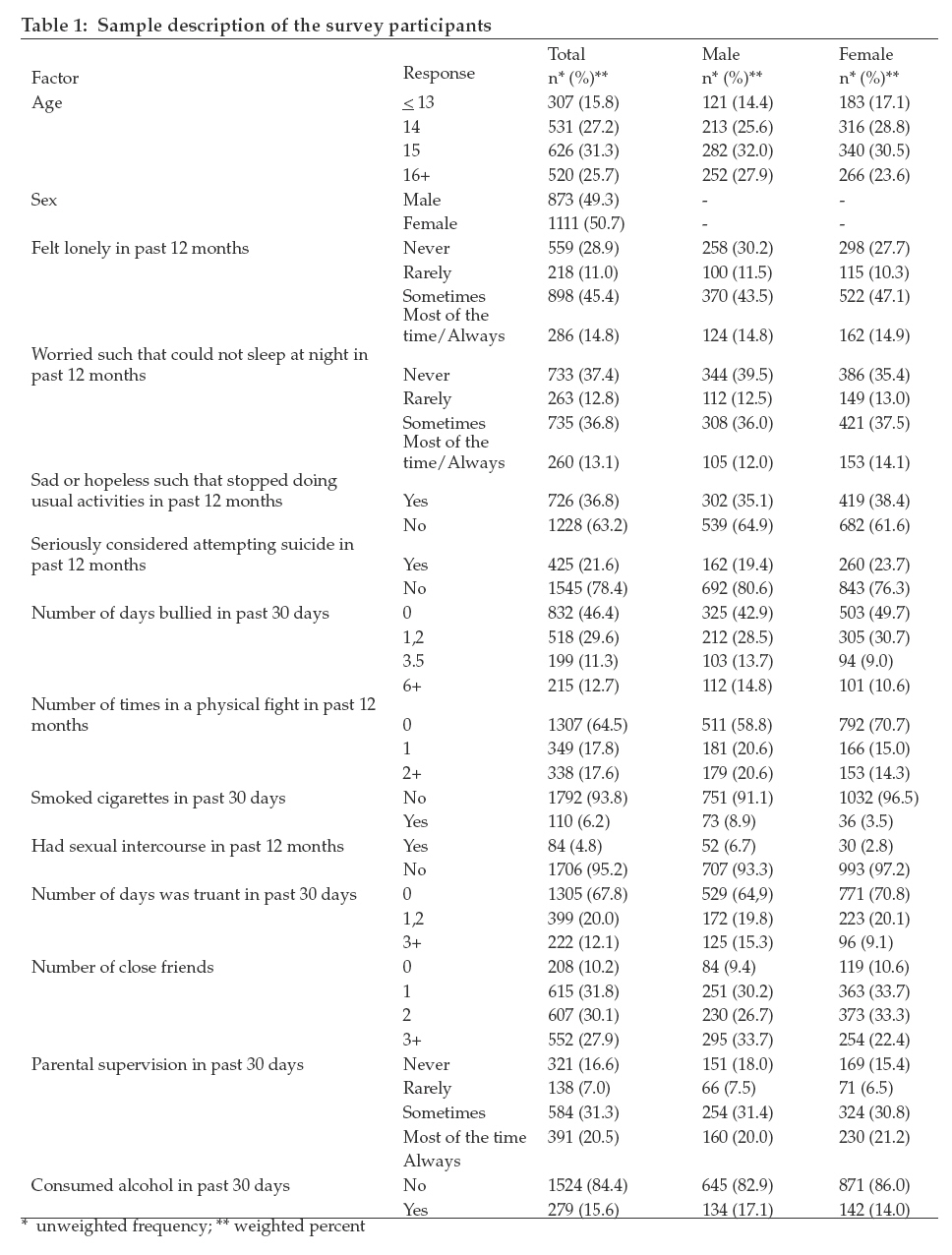
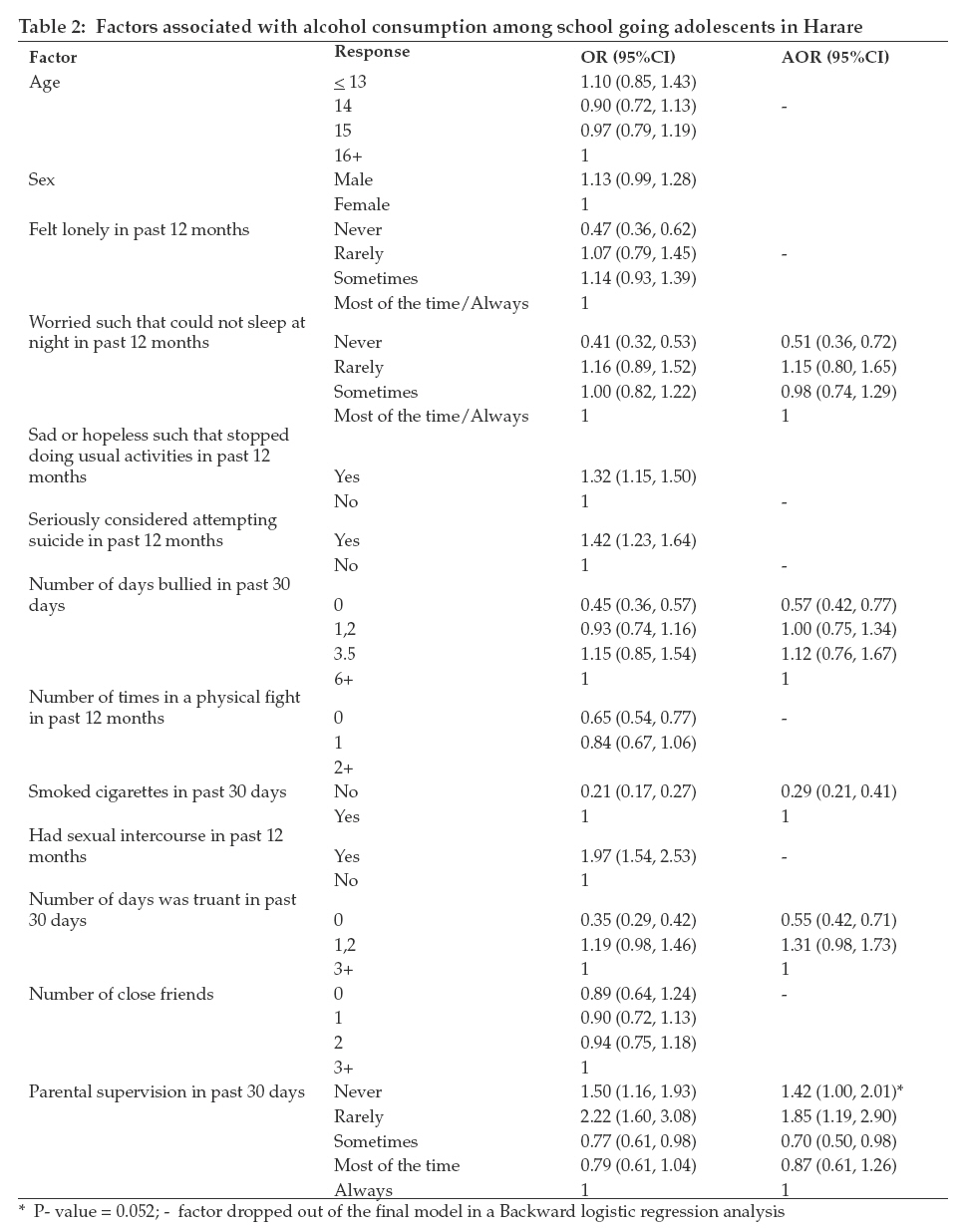
Tanzania Journal of Health Research, Vol. 11, No. 1, January, 2009, pp. 11-16 Alcohol use among school-going adolescents in Harare, Zimbabwe: results from the 2003 Global School-Based Health Survey S. Siziya1, E. Rudatsikira2 and A.S. Muula3* 1 Department of Community Medicine, University of Zambia, School of Medicine, Lusaka, Zambia Code Number: th09003 Abstract Data from the Global School-Based Health Survey (2003) were analysed to estimate the proportions of relevant socio-demographic and behavioural characteristics. Of the 1997 students who participated in the survey, 15.6% (17.1% males and 14.0% females) reported alcohol consumption. Factors associated with consumption of alcohol use were being worried, bullied, smoking cigarettes, truant, and lack of parental supervision. Students who were never worried were 49% (AOR=0.51 [95%CI (0.36, 0.72)]) less likely to consume alcohol compared to students who were most of the time or always worried. Similarly, students who were never bullied were 42% (AOR=0.57 [95%CI (0.42, 0.77)]) less likely to take alcohol compared to students who were bullied at least six times in the previous one month to the survey. Compared to students who smoked cigarettes, non-smokers were 71% (AOR=0.29 [95%CI (0.21, 0.41)]) less likely to consume alcohol. Compared to students who always received parental supervision, students who rarely received parental supervision were more likely (AOR=1.85 [95%CI (1.19, 2.90)] to consume alcohol, and those students who sometimes received parental supervision were less likely (AOR=0.70 [95%CI (0.50, 0.98)] to consume alcohol. There is a need to implement public health interventions with special attention to the determinants of alcohol consumption in this age group. Key words: alcohol use, behaviour, school adolescent, Zimbabwe Introduction In the most recent World Health Organization (WHO) Global Burden of Disease report, it was stated that better epidemiological data on substance use were needed, particularly in less established market economies (Degenhardt et al., 2004; Ezzati & Lopez, 2004). The paucity of data on substance use and an understanding of the relevant risk factors and policy measures are likely to continue due to lower priority that non-communicable diseases garner when compared to infectious diseases. Only two African countries (Nigeria and South Africa) participated in the World Mental Health Survey (WMHS), an initiative of the WHO with the aim of documenting, among other things a comprehensive picture of substance use patterns across the world. The countries which participated in the WMHS were those who had collaborators in the country and were able to obtain funding for the survey. The other 15 countries were Colombia, Mexico, the United States in the Americas, Belgium, France, Germany, Italy, Netherlands, Spain, Ukraine in Europe, Israel and Lebanon in the Middle East, Japan and China in Asia and New Zealand in Oceania. Despite the limited geographical spread of well conducted surveys on substance use especially in Africa, some data are available in selected countries on use among school going adolescents. The Global Tobacco Surveillance Systems’ Global Youth Tobacco Survey (GYTS) and the Global School-Based Health Survey (GSHS) have been key in reducing the lack of knowledge on substance use in African countries. In a study of rural secondary school students in Zimbabwe, Gwede et al. (2001) reported 29.3% and 19.3% lifetime use and previous 30 day use of alcohol, respectively, among the respondents. Males were more likely to have used alcohol than females. In an earlier study of teachers reported by Eide & Acuda (1999), the teachers had reported that alcohol use was the most common substance used in Zimbabwe, followed by cannabis, tobacco, inhalants and other drugs. In a related paper, these authors reported that 38.6% of male teachers and 8.2% of female teachers reported drinking every day or at least weekly (Eide et al., 1999a). It is important that we understand the prevalence and associated factors of alcohol use among adolescents. Adolescents who use alcohol may also be engaged in other unhealthy and antisocial behaviors such as unprotected sexual intercourse, tobacco smoking, violence behaviors and truancy (Santelli et al., 1998; Valois et al., 1999). Furthermore, many adolescent substance users continue doing so into adulthood (Pitkänen et al., 2008; Poikolokainen et al., 2001). Clark et al. (2008) have reported that adolescent-onset substance use disorders prospectively predicted early mortality. In order to contribute to the literature on alcohol use among adolescents in Zimbabwe, we analyzed data from the Harare (the capital city of Zimbabwe) Global School-Based Survey, 2003. The aim of our analysis was to estimate the prevalence of alcohol use, and assess its associated factors. We argue that public health interventions that are designed and implemented having considered the epidemiology of alcohol use, are more likely to be effective than if such considerations are not made. Materials and Methods Several authors have previously reported the details about the GSHS (Brown et al., 2008). In brief however, the GSHS is a self-administered, school-based survey that was developed by the WHO in collaboration with the United Nations Children’s Fund (UNICEF), the United Nations Educational, Scientific and Cultural Organization (UNESCO), and the Joint United Nations Programme on HIV/AIDS (UNAIDS). Technical and financial assistance was obtained from the US Centers for Disease Control and Prevention (CDC). The survey is aimed at recruiting students aged 13–15 years, and a questionnaire is completed within one regular class period. In each country where the survey is administered, the questionnaire comprises multiple core questionnaire modules, coreexpanded questions and country-specific questions. A standardized scientific sample selection process and common school-based methodology is implemented. The survey employed a two-stage cluster sample design to obtain a representative sample of students in forms one to three. In the first-stage of sampling, sampling frame consisted of all schools in Harare containing any of the secondary forms one to three. Forms one to three classes were selected because they contained the majority of the target groups i.e. 13 to 15year age groups, within the schools. Schools were selected with probability proportional to school enrollment size i.e. a school with a larger enrollment had a higher probability of being selected than another with a lower school enrollment. A total of 25 schools were eventually selected as eligible to participate in the study. Using a random start, the second stage of sampling consisted of randomly selecting classrooms. All classrooms selected in the stage one were included in the sampling frame. All students in the sampled classrooms were eligible to participate in the survey. A self-completed questionnaire, using multiple-choice questions, was administered in English. Questionnaires were completed at school within one class period. Protection of the student’s privacy is made through anonymous and voluntary participation. To further help protect student privacy, no skip patterns were allowed. Data were analysed using SPSS version 14.0. We estimated the proportions of relevant socio-demographic and behavioural characteristics. The main outcome of interest was having used alcohol in the 30 days preceding the survey. The question was: ‘During the past 30 days, on how many days did you have at least one drink containing alcohol?’ Weighted analysis initially with single predictor, and then Backward logistic regression in a multivariate model was conducted. We report unadjusted Odds ratios (OR), and Adjusted Odds Ratios (AOR) with their 95% Confidence Intervals (CI). Results Characteristics of survey participants Altogether 1997 students participated in the survey. About a third (31.3%) of the students was of age 15 years, and 49.3% were males. The proportion of students who seriously considered attempting suicide was 21.6%, and that for students who reported being bullied at least once was 53.6%. Overall 6.2% of the students smoked cigarettes. Alcohol consumption was reported by 15.6% of the students (17.1% among males, and 14.0%v among females) (Table 1). Factors associated with alcohol use among adolescents in Harare Age, sex, and number of close friends were not significantly associated with alcohol consumption in bivariate analyses. Bivariate analyses showed that students who were never lonely, never worried, not bullied, not involved in a physical fight, non-smokers, and not truant were less likely to consume alcohol. Factors that were positively associated with alcohol intake in bivariate analyses were being sad or hopeless, seriously considered attempting suicide, having had sexual intercourse, and rarely or never had parental supervision (Table 2). Factors that were independently associated with consumption of alcohol were being worried, bullied, smoking cigarettes, truant, and parental supervision. Students who were never worried were 49% (AOR=0.51 [95%CI (0.36, 0.72)]) less likely to consume alcohol compared to students who were most of the time or always worried. Similarly, students who were never bullied were 42% (AOR=0.57 [95%CI (0.42, 0.77)]) less likely to take alcohol compared to students who were bullied at least six times in the previous one month to the survey. Compared to students who smoked cigarettes, non-smokers were 71% (AOR=0.29 [95%CI (0.21, 0.41)]) less likely to consume alcohol. Students who were not truant were 45% (AOR=0.55 [95%CI (0.42, 0.71)]) less likely to consume alcohol compared to students who were truant at least 3 days in the previous one month to the survey. While students who rarely received parental supervision were more likely (AOR=1.85 [95%CI (1.19, 2.90)] to consume alcohol compared to students who always received parental supervision, those students who sometimes received parental supervision were less likely (AOR=0.70 [95%CI (0.50, 0.98)] to consume alcohol. Discussion In a study of school-going adolescents in Harare, Zimbabwe, we found that in the past 12 months 14.8% of the students felt lonely most of the time or always, 13.1% could not sleep because of worries, while 21.6% had seriously considered committing suicide. The 30 days reported prevalence of using alcohol was 15.6% overall; 17.1% and 14.0% among males and females, respectively. In assessing factors that could be associated with alcohol use, we found that increased number of days that the teen had been bullied, lack of parental supervision most of the times and worry were positively associated with having used alcohol. Non-smokers were less likely to have used alcohol in the past 30 days. Our results conform previous finding as to the factors associated with adolescent alcohol use. In a pooled analysis of GSHS data from 8 African countries, Brown et al. (2008) reported strong associations between bullying among youth and current alcohol use. Parental supervision of adolescents has been previously reported as protective against unhealthy behaviors among adolescents. It has been reported that parental supervision of adolescents may be protective against risky sexual behaviors (Rupp and Rosenthal, 2007). Despite the use of a standardised research protocol, our study has a number of limitations. Perhaps importantly, we can not assign causation to any of the variables, e.g. just because bullying was associated with having used alcohol does not confirm that bullying victimization causes alcohol use. However, bullying could be stressful to the adolescent who may later engage in alcohol use as a way of coping with the stress. It is also possible that adolescents who take alcohol may frequently visit places where bullying is more likely to occur. However, we can only point to the associations without assigning any temporal sequence and causation. Secondly, data were obtained through self-reports and alcohol use was not verified by any of the available biomarkers. To the extent that survey participants mis-reported, either intentionally or non-intentionally, our findings may be biased. However, the GSHS methodology attempts to encourage truthful reporting by self-reporting (instead of being asked questions by an interviewer) and by not collecting any personal identifiers of study participants. This study also was restricted to data from Harare (the capital city) and may not be representative of the rest of the country. Finally, these data were collected from school-going adolescents and therefore may not be representative of all adolescent in the city. In conclusion, prevalence of alcohol consumption among school-going adolescents in Harare, Zimbabwe is similar to what is reported from other African countries. There is a need to implement public health interventions with special attention to the determinants of alcohol consumption in this age group. Acknowledgements We thank the World Health Organisation (WHO) for making these data available to us for analysis. However, neither the WHO nor the Centers for Disease Control and Prevention participated in the decision to analyse these data, our methods or decision to submit manuscript. Grateful thanks to all students and survey assistants who participated in the Harare, Global School Based Survey, 2003. References
© Copyright 2009 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th09003t1.jpg] [th09003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}