 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
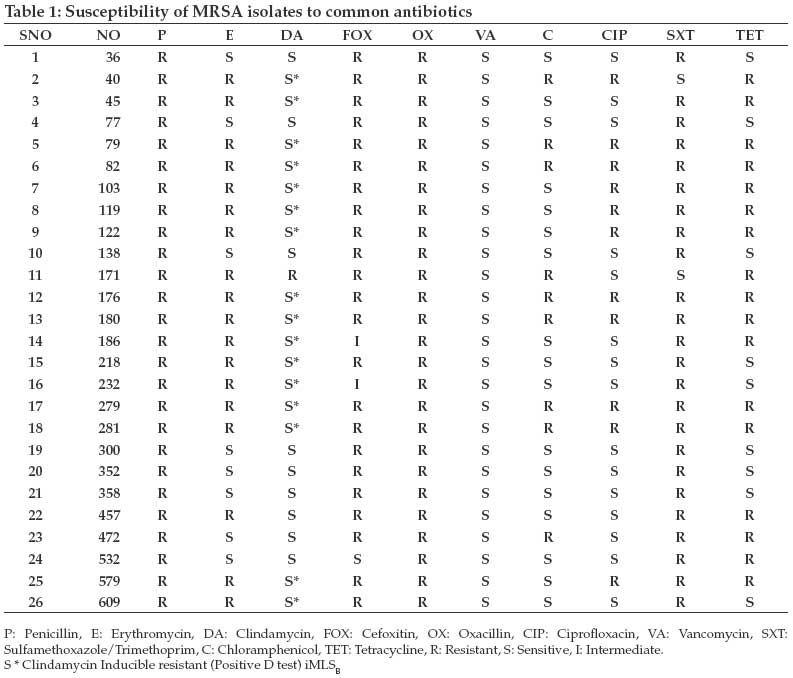
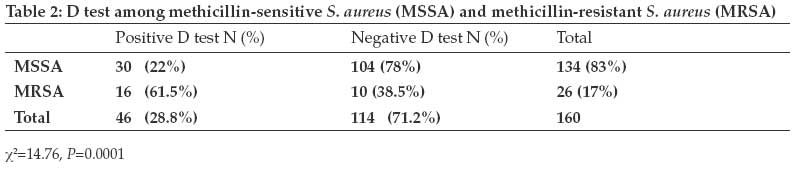
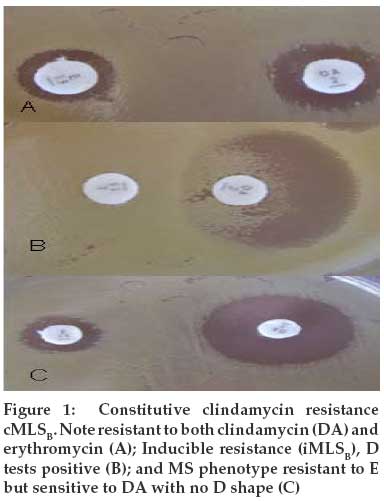
Tanzania Journal of Health Research, Vol. 11, No. 2, April-June, 2009, pp. 59-64 Original Article Prevalence of clindamycin inducible resistance among methicillin-resistant Staphylococcus aureus at Bugando Medical Centre, Mwanza, Tanzania Mshana SE, Kamugisha E, Mirambo M, Chalya P, Rambau P, Mahalu W, Lyamuya E Weill Bugando Medical College of Health Sciences, P.O. Box 1464, Mwanza Correspondence Address:Weill Bugando Medical College of Health Sciences, P.O. Box 1464, Mwanza mshana72@yahoo.com Date of Submission: 04-Nov-2008 Date of Decision: 09-Jan-2009 Date of Acceptance: 10-Jan-2009 Code Number: tj09011 Abstract Methicillin-resistant Staphylococcus aureus (MRSA) has been recognized world wide as an important causative agent of nosocomial and community acquired infections. Clindamycin has been considered as an alternative drug for the treatment of such strains. However, the possibility of clindamycin inducible resistance complicates the choice of treatment. The aim of this study was to determine the prevalence of clindamycin inducible resistance of MRSA at Bugando Medical Centre (BMC) in Mwanza Tanzania. A total of 600 clinical specimens of pus, wound swabs and aspirates from patients admitted at BMC surgical wards were processed over a period of 4 months. Of these, 160 of S. aureus clinical isolates analysed. MRSA was identified using cefoxitin disc, oxacillin disc and oxacillin agar. Inducible clindamycin resistance was detected using erythromycin (15µg) and clindamycin (2µg) discs placed 15mm apart on Muller Hinton agar. Of the 160 isolates, 26 (16.3%) were found to be MRSA. Overall prevalence of inducible clindamycin resistance (iMLS B ) was 28.8% (46/160), with 22% (30/134) of methicillin-susceptible S. aureus (MSSA) and 61% (16/26) of MRSA exhibiting inducible clindamycin resistance ( P= 0.0001). Constitutive resistance (cMLS B ) was found in 1 (3.7%) of the MRSA isolates and was not detected among MSSA. MS B phenotype was detected in 1 (3.8%) of MRSA isolates and 2 (1.5%) of MSSA. Eight (29.6%) of the MRSA isolates were sensitive to both clindamycin and erythromycin. In conclusion, a high prevalence of inducible clindamycin resistance was observed among S. aureus with significant association between MRSA and inducible clindamycin resistance. It is important that susceptibility test of staphylococci is routinely done to facilitate early detection of clindamycin inducible resistance in the country.Keywords: prevalence, clindamycin, methicillin-resistant, Staphylococcus aureus , Tanzania Introduction Staphylococcus aureus has been recognized world wide as an important causative agent of nosocomial and community acquired infections (Jan et al., 2002 ). The increase of methicillin resistant S. aureus (MRSA) among staphylococci is an increasing problem and clindamycin is considered to be one of the potent alternative agents available to address this problem (Fokas et al., 2005). In the USA, Canada and Europe, available statistics indicate that MRSA accounts for up to 40% of nosocomial S. aureus infections in large hospitals and 25%-30% of such infections in smaller hospitals (Jan et al., 2002 ). Epidemiological data on MRSA and inducible clindamycin resistance are scarce in Africa. The prevalence of MRSA in eight countries from 1996 to1997 was reported to be relatively high (21-30%) in Nigeria, Kenya and Cameroon and low (10%) in Tunisia and Algeria (Kesah et al., 2003). Few reports of the antimicrobial susceptibility of S. aureus in Tanzania are available. In a study at the Muhimbili National Hospital in Dar es Salaam, Tanzania, Urassa et al . (1999) observed a 0.4% prevalence of methicillin resistant S. aureus . Recently, at the same hospital, 12% of S. aureus were found to be resistant to cloxacillin (Bloomberg et al., 2007). Macrolide resistance is increasing worldwide. Forinsancd, inducible resistance has been found to be more than 50% in MSSA and constitutive phenotype resistance more than 80% in MRSA (Lina et al., 1999). Inducible clindamycin resistance was reported in 10.8% in MSSA and 82% in MRSA in South Africa (Adebayo et al., 2006). Emergence of resistance to clindamycin in staphylococci shortly after therapeutic use of erythromycin has been reported ( Gopal Rao , 2000 ) . Resistance to macrolides, lincosamides and streptogramin B (MLS antibiotics) is mainly due to acquisition of erythromycin resistant methylase (erm) gene, which encodes enzyme that methylate the 23rRNA ( Fokas et al., 2005 ) . Constitutive resistance phenotype is resistant to macrolides, lincosamides and streptogramin-B but inducible resistance is expressed in the presence of methylase synthesis inducer like erythromycin (14 rings) and azithromycin (15 rings) macrolides (Gopal Rao , 2000). Data on inducible clindamycin resistance among MRSA in Tanzania is not available. This study was therefore carried out to determine the prevalence of MRSA and inducible clindamycin resistance among S. aureus isolates from patients admitted at Bugando Medical Centre in Mwanza, Tanzania. Material and Methods Study area The study was done at Bugando Medical Centre (BMC) in Mwanza, in north-western Tanzania. It is situated along the shores of Lake Victoria and has 900 bed capacity. BMC is a consultant and teaching hospital for the Lake and Western zones of the Tanzania Laboratory protocol A total 600 clinical specimens (pus, wound swabs, aspirates) from patients admitted at BMC surgical wards were processed over a period of 4 months (April-July 2008). All specimens were inoculated on sheep blood agar, MacConkey agar (OXOID UK) and incubated at 37 0 C aerobically for 24h. Identification of S. aureus was first done using colony morphology on 5% sheep blood agar. Cream to golden yellow colonies with or without haemolysis were further identified using Gram stain and catalase test; followed by staphylase and DNAse tests (Murray et al., 1995). Staphylase test (OXOID UK) was done and interpreted as recommended by the manufacturer. DNAse test was done by pouring 1N HCl to the overnight colonies on DNAse test agar (OXOID, UK). Clearance of precipitated DNA around the colonies was reported as positive (Murray et al., 1995) . MRSA detection was done using cefoxitin, oxacillin discs (OXOID UK) and oxacillin screen agar (5% NaCl, 6ìg/ml oxacillin) as described previously ( Murray et al., 1995; Saxena et al., 2003 ) . Bacterial colonies were suspended in saline to a turbidity of 0.5 McFarland standards and inoculated on a Muller Hinton agar plate (OXOID UK). Plates were incubated at 37 0 C for cefoxitin disc and at 33 0 C in the case of oxacillin disc and oxacillin agar. All isolates resistant to cefoxitin and oxacillin were considered as MRSA and its correlation to the presence of mecA gene is more than 95% (Felten et al., 2002; Saxena et al., 2003; Swenson et al., 2005) . Clindamycin inducible resistance was detected as described previously. Erythromycin (15µg) and clindamycin (2µg) (OXOID UK) discs were placed 15-20mm apart edge to edge (Adebayo et al., 2006; Delialioglu et al., 2005; Ravisekhar et al., 2006). Appearance of flattened clindamycin zone between clindamycin and erythromycin forming D shape with erythromycin resistance was considered as positive clindamycin inducible resistant (iMLS B ). Resistance to both discs was recorded as constitutive resistance (cMLS B ) and resistance to erythromycin alone was taken as MS phenotype. Interpretation of the diameters of zone inhibition was as follows: Erythromycin (E)-sensitive (S) = ≥ 23mm, E-Intermediate (I) =14 to 22mm, E-resistance = ≤ 13mm; Clindamycin (DA)-S= ≥21mm, DA-I=15-20 mm, DA-R = ≤14mm (Fokas et al., 2005; CLSI 2000). Disc susceptibility testing for penicillin (10IU), oxacillin (1µg), cefoxitin (30µg), vancomycin (30µg), ciprofloxacin (5µg), chloramphenicol (30µg), tetracycline (30µg) and sulfamethaxazole/trimethoprim (25µg) (UK OXOID) was done using standard procedures (CLSI, 2000). For the quality control of media, incubation conditions and discs and Escherichia coli strain ATCC 25922 from Mwanza Medical Research Centre of the National Institute of Medical Research was used. Results Among 600 non-repetitive clinical specimens 160 (26.6%) S. aureus were isolated. Methicillin-resistant S. aureus were identified in 26 (16.3%) of all S. aureus isolates. Almost all 155/160 (97%) of S. aureus isolates were resistant to penicillin and all the S. aureus isolates were sensitive to vancomycin. Rates of resistance to chloramphenicol, ciprofloxacin, tetracycline and sulfamethaxazole/trimethoprim among MRSA were 10 (39%), 14 (54%), 18 (69%) and 24 (92%), respectively [Table - 1]. Overall prevalence of inducible clindamycin resistance (iMLS B ) was 46(28.8%), with 30/134 (22%) of methicillin-susceptible S. aureus (MSSA) and 16/26 (61.5%) of MRSA exhibiting inducible clindamycin resistance Table - 2. There was significant association between MRSA and inducible clindamycin resistance (iMLS B ) among staphylococci isolates (×2 = 14.75, P =0.0001 Table - 2. Constitutive resistance (cMLS B ) was found in 1 (3.7%) among MRSA isolates and was not detected among MSSA. Among MRSA isolates resistance to erythromycin alone with negative D test (MS B phenotype) was detected in 3.8% of the isolates and 1.5% of MSSA isolates Figure - 1. Eight (29.6%) of MRSA isolates were found to be sensitive to both clindamycin and erythromycin. All MRSA isolates were preserved for future molecular analysis. Discussion In the present study S. aureus was commonly isolated from surgical patients (26.6%). Similar observations have been reported elsewhere that S. aureus is the cause of most wound infections among hospitalized patients (Jan et al., 2002; Bloomberg et al., 2007). Only 3.1% of the isolates were sensitive to penicillin, possibly due to production of â-lactamases enzyme which hydrolyzes penicillin. Similar findings have been reported recently at the Muhimbili National Hospital in Dar es Salaam where as high as 100% of S. aureus isolates were reported to be resistant to penicillin (Bloomberg et al., 2007). In our study using disc diffusion method the resistance to oxacillin and cefoxitin which signifies MRSA was observed in 16.2% of isolates. Disc diffusion especially oxacillin disc has been used in most developing countries to detect MRSA (Felten et al., 2002). In developed countries MIC methods has been replaced by molecular methods that detect mecA gene (Brown et al ., 2001). Use of cefoxitin disc have been found to have high correlation (>95%) with the presence of mecA gene (Felten et al., 2002; Swenson et al., 2005). In few cases where the low resistance to oxacillin and cefoxitin does not correlate to the presence of mecA gene disc variation and hyperproduction of penicillinase can explain the discrepancy (Chambers et al., 1990; Yassin et al. , 1997). Our findings are similar to those reported from the Muhimbili National Hospital study where 12% of hospital isolated S. aureus were resistant to cloxacillin (Bloomberg et al., 2007). This is yet, relatively lower prevalence compared to the findings in elsewhere, 24-74% of the S. aureus were MRSA (Jan et al., 2002; Adebayo et al., 2006). Clindamycin is a useful drug in the treatment of both methicillin susceptible and resistant staphylococcal infections. In our study clindamycin inducible resistance (iMLS B ) was observed in 61% and 22% of MRSA and MSSA, respectively. Similarly, a study in Kwa-Zulu Natal in South Africa has indicated that 10.8% of MSSA and 82% of MRSA had inducible clindamycin resistance. Other studies conducted elsewhere have reported high prevalence of clindamycin inducible resistance among MSSA (Ravisekhar et al., 2006; Patel et al., 2006 ) . A significant association between MRSA and inducible clindamycin resistance and the presence of MS phenotype in both MSSA and MRSA was observed in our study. Recent studies in Turkey and Nepal have detected MS phenotype only in MSSA (Fokas et al., 2005; Azap et al., 2005). In the present study, the constitutive clindamycin resistance was identified in one MRSA isolate and was absent in all MSSA. This trend is in contrast with other studies in Korea where the majority of MRSA had constitutive resistance (cMLS B ) (Kim et al., 2004). This indicates that the incidence of constitutive and inducible resistance in staphylococcal isolates is likely to vary by regions. Moreover, the low constitutive clindamycin resistance in our study may also be due to the fact that the drug is not commonly used, and hence there is less selection of resistant strains. The development of resistance to antibiotics is related to the wide-spread use of the respective antibiotic ( Yajarayma et al., 2005 ) . To the best our knowledge this is the first study describing clindamycin inducible resistance among MRSA and MSSA in Tanzania. Our findings indicate that the majority of MRSA isolates were resistant to sulfamethoxazole/trimethoprim. Similar observations have been reported in South Africa (Adebayo et al., 2006) . As in other studies all MRSA isolates were sensitive to vancomycin and chloramphenicol. Chloramphenicol can be used in our setting for non serious MRSA infection and in case of bacteraemia vancomycin is recommended (Jan et al., 2002; Bloomberg et al., 2007). One-third of MRSA isolates and three quarters of MSSA were sensitive to both erythromycin and clindamycin. The drugs therefore, can still be used for non-serious staphylococcal infections in the study area. However, it is important that this is guided by culture results. In conclusion, high prevalence of inducible clindamycin resistance was observed among S. aureus isolates, with significant association between MRSA and inducible clindamycin resistance. It should be noted that the results of this study represent S. aureus from a single hospital and may not be a representative of the rest of the country. Since it is likely that the prevalence of iMLS B and MRSA clones differs from region to region, it is recommended that clinical microbiology laboratories should routinely include disc diffusion induction tests to facilitate detection of clindamycin inducible resistance (iMLS B ) in the country. The need to establish antimicrobial resistance surveillance in the tertiary care facilities in Tanzania to track the mergence of drug resistant bacterial agents is also strongly recommended. Acknowledgements We thank Mary Louise Shushu, Sifael Msuya, Hezron Bassu and Bella Evans for their excellent technical assistance. The Director, Mwanza Medical Research Centre is thanked for providing the incubation condition and E. coli strains. This work was supported from research grant of the WBUCHS to S.E.M.[22] References
Copyright 2009 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th09011t2.jpg] [th09011t1.jpg] [th09011f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}