 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
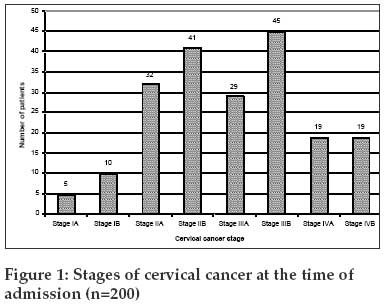
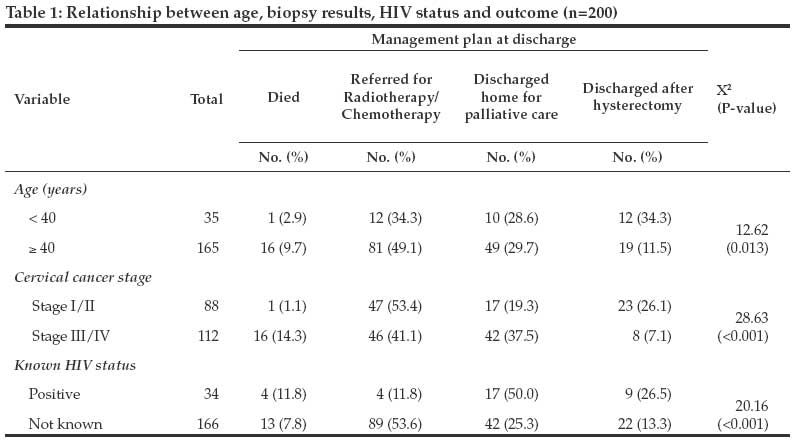
Tanzania Journal of Health Research, Vol. 11, No. 2, April-June, 2009, pp. 70-74 Original Article Factors associated with management of cervical cancer patients at KCMC Hospital, Tanzania: A retrospective cross-sectional study Mosha D, Mahande M, Ahaz J, Mosha M, Njau B, Kitali B, Obure J Kilimanjaro Christian Medical College, P.O Box 2240, Moshi Correspondence Address:Kilimanjaro Christian Medical College, P.O Box 2240, Moshi dfmosha@hotmail.com Date of Submission: 29-Dec-2008 Code Number: th09013 Abstract Cervical cancer is an important public health problem among adult women worldwide. It is the second commonest malignancy in female worldwide and the leading malignancy among women in Tanzania. In most developing countries, cancer of the cervix tends to be diagnosed in its later stages when is less treatable. This study aimed at assessing factors associated with management of cervical cancer at KCMC Hospital in northern Tanzania. A purpose sampling was used to select a total of 200 patient records out of 374 with complete information. Median age of cervical cancer patients was 51 years (range 21-84 years) and 81.5% were either married or co-habiting. Stage of the cervical cancer (X 2 = 28.63, p < 0.001) and age (÷2 = 12.62, P <0.05) were significant predictors for patient's management plan, with 56% of cases seen at late cancer stage. Forty-seven percent of the cervical cancer patients were referred to Ocean Road Cancer Institute for radiotherapy and or chemotherapy. Patients discharged home for palliative care were 30% and 17% patients died at the hospital. Known HIV positive patients were significantly associated with death and terminal care seen at late stage than patients with unknown HIV sero-status (X 2 = 20.16, P <0.001). In conclusion, most of cervical cancer patients at KCMC are seen at late stage necessitating referral for radiotherapy, chemotherapy or palliative care. This may reflect lack of cervical screening in order to early detect and treat pre-malignant disease stage.Keywords: Cervical cancer, women, patient management, Tanzania Introduction Cervical cancer is the second most common cancer in women worldwide, comprises approximately 12% of all cancers in women. Worldwide it is estimated that there are 493,000 new cases and more than 274,000 deaths due to cervical cancer each year. Eighty percent of these deaths occur in developing countries, making cervical cancer one of the gravest threats to women lives (Parkin et al., 2005). In Tanzania, the prevalence of cancer of the cervix is still not very clear but it is reported to be the leading malignancy among women (Kahesa et al., 2008). The main reasons for higher incidence of the cervical cancer and its associated mortality in developing countries include lack of awareness of cervical cancer in the general population and health care providers and policy-makers; and lack of effective screening programme to detect and treat pre-invasive diseases stage (Sankaranarayanan et al., 2001). The primary underlying causes of cervical cancer is the persistent infection with potentially oncogenic strains of human papiloma virus (HPV) such as type 16 and 18 that are sexually transmitted (Walboomers et al., 1999). Cervical cancer usually affects women of middle or older age, but it may be diagnosed in any reproductive-aged women especially those infected with HIV/AIDS which enhances HPV proliferation (Moscicki et al., 2000; Strickler et al., 2005). In developing countries, few study reports are available describing the magnitude of cervical cancer, disease stage, management and immediate outcome of theses patients (Walker et al., 1985; Wabinga et al., 2003). Even in these few studies, it has been revealed that the outcome is poor although cancer of the cervix is one of the few cancers which are easily preventable and treatable once diagnosed earlier. For most of the women who have never been screened, cancer of the cervix tends to be diagnosed in its later stages when is less treatable (Baseman & Koutsky, 2005). The aim of this study was therefore to assess factors associated with management of cervical cancer at referral level of health care service and to identify the available treatment modalities of cervical cancer. Materials and Methods Study area The study was carried out at the Kilimanjaro Christian Medical Centre (KCMC) in Moshi, northern Tanzania. KCMC is located in the foothills of Mount Kilimanjaro and is a 450 bed referral hospital for over 11 million people in from Tanga, Kilimanjaro, Arusha, Manyara and Singida regions of Tanzania. Study design and data collection This was a hospital-based, descriptive retrospective cross-sectional study, conducted from June to August, 2008. Included in the study were all patients who were admitted at KCMC Gynaecological Department for their first time with histological diagnosis of cervical cancer in between 2005 and 2007. A purpose sampling was used to collect 200 patients′ files out of 374 with complete information needed for the study. Data was collected using a well-structured checklist containing important study parameters (age, residency, marital status, cancer stage, presenting signs and symptoms, known HIV status, and management plan at discharge). Relevant information was extracted patients′ files to fill in a prepared checklist. Data analysis Data were double entered in MS Access and analysis was done using SPSS version 10. Numerical variables were summarised into median and range. Categorical variables were summarised using cross tabulation to estimate different proportions, ÷2 (and chi-trend) and their respective p-value at 5% (2-tail) was also estimated. Ethical consideration Before conducting this study the ethical approval was obtained from KCMC Ethics Committee. All information from patient′s case notes were kept confidential and were only accessed by the research team. Only individuals′ identification numbers were used instead of patients′ names. Results Records of 200 out of 374 patients admitted for their first time at KCMC gynaecology department with a confirmed diagnosis of cervical cancer were reviewed. Median age was 51.4 (range 21-84 years) years. Majority of the patients, 115 (57.5%) were in the age group of between 40 and 59 years, 50 (25.0%) were aged 60 years and above while 35 (17.5%) aged between 21 and 39 years. There was a wide variation in marital status among cervical cancer cases. A total of 163 (81.5%) were either married or co-habiting, 16 (8.0%) divorced, 15 (7.5%) widows and single were 6(3.0%). Majority (69.0%; N=138) cases of the admitted cervical cancer patients were residents of Kilimanjaro region. Others were from neighbouring regions of Arusha and Manyara (16.0%), Singida (4.5%) and Tanga (3.5%). Fourteen (7.0%) cases came as far as Mara, Dar es Salaam, Tabora, Mbeya, Morogoro, Zanzibar and Kenya. Per vaginal (PV) discharge was the most common symptom reported by all patients. Other symptoms were lower abdominal pain in 199 (99.5%), backache (87.0%), post-coital bleeding (77.5%), post-menopause bleeding (39.0%), dyspareunia (52.5%) and increase frequency of passing urine (9.5%). Macroscopic cervical lesion having white or red patches on cervix was the most common sign picked from nearly all patients (91.5%). Based on International Federation of Gynaecology and Obstetrics classification for staging cervical cancer (ACS, 2008), 88 (44%) patients were admitted with cervical cancer stage I and stage II, 74 (37%) were at stage III and the remaining 38 (19%) had stage IV. Cervical cancer stage I/II were lower in percentage than stage III/IV [Figure - 1]. Patients admitted with cervical cancer stages I and II had a better outcome following abdominal hysterectomy and or chemotherapy. Therefore, cervical cancer staging was a significant factor for predicting patient′s management plan (÷2 =28.63, P< 0.001). Age was an important factor to predict patient′s management plan (÷2 = 12.62, P < 0.05), older women (age 40 years or above) were more likely to die or to be referred to Ocean Road Cancer Institute (ORCI) in Dar es Salaam, for radiotherapy and or chemotherapy than younger women (< 40 years). Thirty percent of the admitted patients were finally discharged home for terminal care and 47% were referred to ORCI in Dar es Salaam for radiotherapy and or chemotherapy. Patients with cervical cancer and known to be HIV sero-positive were more likely to die (11.8% versus 7.8%) or to be discharged home for palliative care (50.0% versus 25.3%) than patients with unknown HIV sero-status. The association between known HIV sero-positive and unknown HIV sero-status was significant predicting factor for patient′s management plan (÷2 = 20.16, P < 0.001). Discussion The geographical distribution shows that majority of patients came from Kilimanjaro, Arusha and Manyara regions. The larger proportion of patients from this regions indicates easy geographical accessibility and does not necessarily signify highest prevalence of cervical cancer in the regions. Furthermore, Tanzania like other many developing countries does not have cervical cancer screening programme and health services do not have capacity or resources to organize and sustain screening programme despite the fact that cervical cancer to account for 80% of new female cancer cases in the country (WHO, 2007). Majority of the admitted patients (58%) were above 40 years old. This findings are consistent with the data from cancer registries in developing countries (Freedman et al., 2006) whereby about 80%-90% of confirmed cervical cancer cases occur in women aged 40s or older. This is because cervical cancer progresses slowly from precancerous conditions to advanced cancer. The incidence of cancer in most countries is very low in women under 35 to 40 years old and reaches a maximum in women of 50s and 60s (Ashford et al., 2005). Age was a significant factor for predicting patient′s management whereby the women aged below 40 years were found to have hysterectomy with less death than those above 40 years. In recent years, some studies have indicated a trend towards age decrease in women with cervical cancer. This is mainly associated with immunosuppression resulting from HIV infection leading to rapidly invasive cancer progression from pre-invasive diseases (Moscicki et al., 2000; Strickler et al., 2005). Despite the fact that our study could not evaluate the association between cervical cancer and HIV, still the likelihood of death or discharged home for palliative care was significantly higher in the known HIV sero-positive women, compared to women with unknown HIV sero-status. Kahesa et al. (2008) have reported similar findings that combination of cancer of the cervix and HIV is usually lethal and many women with these two diseases die before they seek health care Per vaginal discharge was the clinical symptom reported by all patients followed by lower abdominal pain, backache and post coital bleeding. This calls for clinicians to at least perform a speculum examination as a primary screening tool in areas with limited resources for screening cervical cancer. Managing patients with cervical cancer is still a challenging problem in most developing countries due to the reason that most of the women come to seek medical care after they have developed sign and symptoms (Chirenje et al., 2001). Fifty-six percent of the admitted patients presented with cervical cancer at stage III and IV, and these had poor prognosis compared to patients presented at stage I and II. These results are similar to other reports of late diagnosis due to lack of screening services (Wabinga et al., 2003; Ngwelle et al., 2001). Therefore, without access to viable programme, women from poor communities will continue to seek care only when they have developed symptoms and advanced stages of cervical cancer which is difficult to treat. The majority of cases recorded at KCMC were at stages III and IV indicating that most patients were seeking care late stages of the diseases. It is estimated that over 80% of women with cervical cancer in developing countries are diagnosed at advanced stages (Stewart & Kleihues, 2003). In our study, about one-third of the admitted patients were finally discharged home for terminal care and about half were referred to ORCI in Dar es Salaam for radiotherapy and or chemotherapy. Studies elsewhere have indicated that death, palliative care, referred for radiotherapy and or chemotherapy reflect diseases detection at late stage where prognosis is poor (Walker et al., 1985; Wabinga et al., 2003). Although our findings do not represent the situation all over the country and that do not reveal the medium and long-term patient outcomes (Ngwelle et al., 2001; Kahesa et al., 2008; Wabinga et al., 2003) the study provides an indication of the burden of cervical cancer and its immediate outcomes in settings where screening do not exist. Statistics indicate that cervical cancer is preventable by effective screening programmes and considerable reductions in its incidence and death has been recorded in developed countries (Elovainio et al ., 1997). In conclusion, most of cervical cancer patients are seen at an advance disease stage ending with treatment plans associated with poor prognosis or death. We therefore call upon for the comprehensive cervical cancer screening programme by the Ministry of Health for the early detection and prompt treatment of pre-invasive disease. Competing interests The authors declare no competing interest.[15][Table - 1] References
Copyright 2009 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th09013f1.jpg] [th09013t1.jpg] |
| |||||||||

{kind=link}
{kind=link}