 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
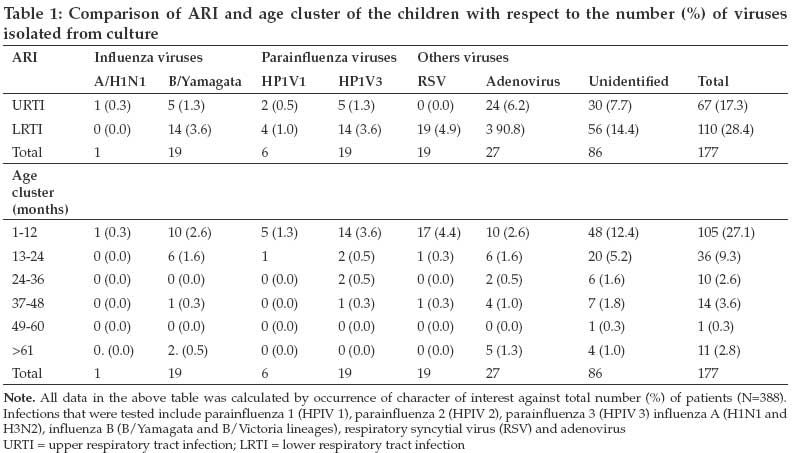
Tanzania Journal of Health Research, Vol. 11, No. 2, April-June, 2009, pp. 90-93 Short Communication Prevalence of viral aetiologies in children with acute respiratory infections in Nairobi, Kenya Symekher S.M.L., Ochieng WO, Simwa J Acute Respiratory Infection Unit, Center for Virus Research, Kenya Medical Research Institute, P.O. Box 54628-00200, Nairobi Correspondence Address:Acute Respiratory Infection Unit, Center for Virus Research, Kenya Medical Research Institute, P.O. Box 54628-00200, Nairobi simorris@kemrinuitm.or.ke Date of Submission: 19-Jan-2009 Date of Decision: 22-Mar-2009 Date of Acceptance: 24-Mar-2009 Code Number: th09017 Abstract Acute respiratory infections (ARIs) are among the leading causes of morbidity and mortality in children under five years in developing countries. Viruses have been long established to be causes of ARIs, but there is little information in developing countries especially Africa. This cross-sectional study was carried out in April-July 2008 in Nairobi, Kenya aiming at establishing which virus isolates and what age cluster in children with ARIs are affected. Throat swabs were collected from patients with clinical ARI and inoculated to various cell lines to isolate and identify viruses. A total of 388 children (age range = 1-132 months) were recruited. Of these 210 (54.1%) were males and 178 (45.9%) were females. Twenty-six percent (101) had upper (URTI) while 74% (287) had lower (LRTI) respiratory tract infections. There were 177 (45.6%) viruses isolated; adenovirus (27; 7%), parainfluenza (25; 6.4%), influenza (20; 5.2%), respiratory syncytial virus (19; 4.9%) and unidentified viruses (86; 22.2%). Majority of the viruses were isolated from patients with LRTI (110; 28.4%) while URTI had 67 (17.3%) isolates. The age cluster 1-12months (105; 27.1%) followed by 13-24months (36; 9.3%) had majority of the viral isolates. Thus this study indicates that viruses are associated with ARIs in children 1-2years of age and therefore a longitudinal study with sensitive virus detection methods is required to provide more information on the precise disease burden and magnitude of the problem.Keywords: Acute respiratory infections, viruses, children, Kenya Disease surveillance plays an integral part in public health by providing early and precise information on key aspects of disease activity such as time, location, disease agent type, and disease severity. It is through such activities that a cute respiratory infections (ARIs) which are divided into upper respiratory tract (URTI) and lower respiratory tract infections (LRTI), has been established as one of the leading causes of childhood morbidity and mortality. Children under five years may experience three to six episodes of ARIs annually regardless of their socio-economic status (Simoes et al., 2006). Estimates indicate that up to 1.9 million children die each year from ARI with about 70% of these deaths occurring in Africa and South East Asia (Simoes et al., 2006). Some of the URTI include rhinitis (common cold), sinusitis, ear infections (Otitis Media), acute pharyngitis or tonsillopharyngitis, epiglotitis and laryngitis. The most common LRTI in children are pneumonia and bronchiolitis (Simoes et al. , 2006). Literature indicates that ARIs could be caused by either or a combination of both bacterial (e.g. Streptococcus pneumoniae and Haemophilus influenza ) or viral agents (such as influenza, metapneumovirus, parainfluenza, respiratory syncytial virus, and adenovirus). Since the establishment of viral isolation, a number of studies have indicated that viruses are important causes of upper and lower respiratory tract diseases in infants and young children and are therefore of public health importance (van Woensel et al. , 2003; van Gageldonk-Lafeber et al. , 2007). The role of viruses in the aetiology of ARI in developing countries especially Africa is not well studied. The information on virus isolates associated with ARI is important in designing appropriate ARI control strategies including patient management, vaccination programmes, antimicrobial and antiviral therapy. The aims of this study were to determine which viruses are associated with ARI (both upper and lower respiratory tract infections) in children at Kenyatta National Hospital, a national referral hospital in Nairobi Kenya, and what age bracket was most affected by ARI. This was a cross-sectional study carried out between April-July 2008. Purposeful sampling was carried out where throat swabs were collected from all children presenting with ARI, who were included after consent was sought and obtained from the parents of those eligible children. After collecting the sample, the swab was inserted into a cryovial containing virus transport medium (VTM) and transported within 2 to 4 hours in a cool box to the Acute Respiratory Infections Unit of the Center for Virus Research, Kenya Medical Research Institute for virus isolation and identification. Once the samples were received, they were recorded and stored in a -80 0 C freezer until the day they were processed for inoculation to cell lines for virus isolation. Samples were thawed and kept in ice prior to inoculation. One hundred microlitres (100µl) of the sample was inoculated to all cell lines (MDCK, LLCMK2 and HEP-2) that had been prepared in 24 well plates and incubated for 1 hour at 35 0 C for virus adsorption. Maintenance medium was overlaid to cells (LLCMK2 and MDCK maintenance medium contained 0.25% trypsin while HEP-2 cells maintenance medium did not have trypsin) and incubated at 33 0 C for up to 12 days. The tubes were examined everyday to detect any contamination or cytopathic effect (CPE). Once CPE was observed on either cell line, the samples were frozen at -80 0 C in preparation for virus identification. If CPE was seen on MDCK cell line, haemagglutination (HA) and haemagglutination inhibition (HAI) assays were performed to identify influenza viruses. If CPE was seen in any other cell line, the sample was prepared to be stained using Simulfluor reagent (Chemicon international, California), a direct fluorescent test (DFT) performed using specific monoclonal antibodies conjugated with a fluorescent dye flourescein isothiocyanate (FITC) and examined under an Olympus fluorescent microscope. Adenovirus, respiratory syncytial virus (RSV), and parainfluenza types 1, 2 and 3 were tested using DFT. A total of 388 patients were recruited during the study period. Of the patients recruited 210 (54.1%) were males while 178 (45.9%) were females. All patients recruited had clinically diagnosed ARI that was either classified as URTI (n= 101; 26%) or LRTI (n = 287; 74%). The age range of the patients was between 1 month and 132 months with majority of the patients being in the 1-12 month age cluster (251; 64.7%), followed by the 13-24 month (68; 17.5%), then both the 25-36 and 37-48 month age clusters (23; 5.9%), the more than 61 months age cluster (16; 4.1%), and lastly the 49-60 month age cluster (7; 1.8%). There were a total of 177 (45.6%) viruses isolated from the patients recruited in the study. Of the viruses isolated 20 (5.2%) were influenza (1; 0.3% influenza A/H1N1 and 19; 4.9% influenza B/Yamagata), 25 (6.4%) were parainfluenza (6; 1.6% HPIV1 and 19; 4.9% HPIV3), 19 (4.9%) RSV, 27 (7%) adenovirus, and 86 (22.2%) unidentified viruses [Table - 1]. The study also indicates that viruses were isolated from the patients with ARI. The patients with LRTI (n=110; 28.4%) having the bulk of virus infection when compared with patients with URTI (n=67; 17.3%). The age cluster 1-12 months was most affected (n=105; 27.1%) followed by the 13-24 (n=36; 9.3%) months age cluster. A number of viruses (influenza A/H1N1, B/Yamagata-lineage; parainfluenza 1, 3; RSV; adenovirus and unidentified viruses) were isolated from patients of all age clusters recruited with ARI (either URTI or LRTI). In this study majority of the virus isolations were obtained in the 1-12 and 13-24 month age clusters, which is similar to what has been seen in other studies showing that infections occur in the first two years of a child′s life (van Woensel et al , 2003; Kusel et al , 2007). The most common identified virus isolated was adenovirus, a common causative agent of ARI (Wong, 2007), which in this study it was more common in patients with URTI than LRTI. Adenovirus was isolated from all age group clusters but majority were isolated in the 1-12 month age cluster. This was followed by the human parainfluenza viruses (HPIVs) including HPIV1 and HPIV3 that were isolated mostly from patients in the 1-12 month cluster with LRTI as compared to URTI. The HPIVs have also been shown to cause both infections (URTI and LRTI) in children (Aguilar et al., 2000; Henrickson, 2003). Influenza viruses then followed with majority of the virus isolates being isolated in patients aged between 1-12 and 13-24 months who had been diagnosed with LRTI when compared to URTI. This was followed by RSV which was only isolated in patients with LRTI and in the 1-12 month age cluster. This is similar to other studies which showed that RSV is major cause of LRTI (Ajayi-Obe et al. , 2008; Woensel et al. , 2003). There are differences in the proportions of virus isolates when this study is compared to the study carried out by Hazlett et al. (1998). While this study had more isolates of adenovirus, HPIVs, and influenza, the study by Hazlett et al. (1998) had more RSV isolates. Our study covered part of the year and had limited funds to obtain reagents to identify all viruses and thus the reason why there are many unidentified viruses. A longitudinal study using molecular detection techniques such as polymerase chain reaction and sequencing is required to provide more detailed information on the burden of viruses infecting children to enhance patient management and reduce the morbidity and mortality. Acknowledgements We are indebted to the efforts of Dr. Annette Sang from Kenyatta National Hospital for her contributions in this study. We also acknowledge the Director of Kenya Medical Research Institute, Director of Center for Virus Research (CVR), and CVR staff for facilitating this study. Sanofi Pasteur is thanked for supporting ARI activities by providing the immunofluorescence reagents. We are also grateful to Dr. Ian Barr of the World Health Organization collaborating Centre for Reference and Research in Influenza, Melbourne, Australia for providing the influenza diagnostic reagents.[10] References
Copyright 2009 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th09017t1.jpg] |
| |||||||||

{kind=link}