 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
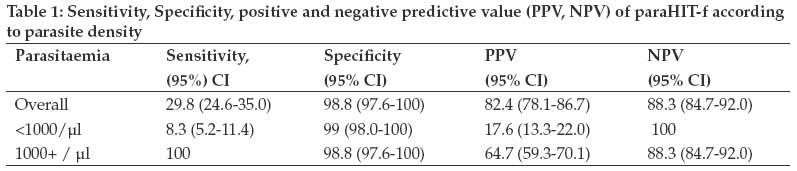
Tanzania Journal of Health Research, Vol. 11, No. 2, April-June, 2009, pp. 97-99 Short Communication Low sensitivity but high specificity of ParaHIT-f in diagnosing malaria among children attending outpatient department in Butimba District Hospital, Mwanza, Tanzania Kamugisha E, Mazigo H, Manyama M, Rambau P, Mirambo M, Kataraihya JB, Mshana S Weill Bugando University College of Health Sciences, P.O. Box 1464, Mwanza Correspondence Address:Weill Bugando University College of Health Sciences, P.O. Box 1464, Mwanza erasmuskamugisha@yahoo.com Date of Submission: 22-Jan-2009 Date of Decision: 23-Mar-2009 Date of Acceptance: 24-Mar-2009 Code Number: th09019 Abstract Malaria is the leading cause of mortality among under-fives in the sub-Saharan Africa. The gold standard method for the diagnosis of malaria is by the use of microscopy which is time consuming and requires skilled technicians. Recently the cost effective antigen based rapid diagnostic tests (RDTs) such as ParaHIT-f have been introduced in various places for the diagnosis of malaria. The choice of these RDTs to use in a certain country and specific geographical locations is critical to malaria diagnosis, treatment and ultimately control of drug resistance. This study was conducted to evaluate the sensitivity and specificity of the cheapest and easily available RDT in the study area, using microscopy as gold standard. This cross-sectional study was conducted to determine the performance of ParaHIT-f in diagnosing malaria in 300 children attending outpatient department at Butimba district hospital. Two thick and one thin blood smear were stained using standard Giemsa stain. The prevalence of P. falciparum Malaria was 5.7% and 15.7% by ParaHIT-f and microscopy respectively; the difference was significant (p<0.001). The sensitivity and specificity of ParaHIT-f were 29.8% and 98.8% respectively. There was a strong association between parasitaemia of ≥1000parasites/µl and being positive for ParaHIT-f diagnostic test (P <0.001). There is a need to revisit the use of ParaHIT-f in Tanzania. Further studies on the sensitivity and specificity are needed. A good quality control system on the performance of ParaHIT-f and other RDTs is highly recommended.Keywords: Malaria, diagnosis ParaHIT-f, sensitivity, specificity, Tanzania Malaria presents a diagnostic challenge in most tropical countries and its diagnosis still relies on clinical presentation and microscopic examination of blood smears. Microscopy is labour intensive, requires significant skills and time which causes delay in treatment and overdiagnosis (Reyburn et al ., 2004). These limitations in diagnosing malaria can lead to fatal complications if not diagnosed and treated at appropriate time (Marsh et al., 1996). Introduction of rapid diagnostic tests (RDTs) is a promising way forward in quick diagnosis of malaria and hence early treatment and reduction of complications (WHO, 2000). There are several studies that have evaluated RDTs in Tanzania (Mboera et al., 2006; Reyburn et al ., 2007; Kamugisha et al ., 2008) and have come up with promising results. Worldwide results of different RDTs have differed a lot, with some reporting higher sensitivities and specificities while others reporting the opposite (Kamugisha et al., 2008; Belizario et al., 2005). The availability and cost of RDTs are among factors that determine which RDTs will be used in a particular setting. There is a need to evaluate the locally available RTD kits in the markets that are likely to be used in malaria diagnosis. This study was therefore carried out to compare ParaHIT-f with microscopy in diagnosing malaria among children at the outpatient clinic at Butimba District Hospital in Mwanza, Tanzania. A cross-sectional study was conducted from June to July, 2008 to determine the performance of ParaHIT-f in diagnosing malaria in 300 children. All children aged between 1 and 120 months who attended outpatient department with history and clinical features suggestive of malaria were recruited serially until the sample size was reached. A finger-prick blood sample was collected aseptically after obtaining a written informed consent from caregivers. The sample was used to prepare blood smears and for testing with ParaHIT-f test. Two thick and one thin blood smears were stained with 10% Giemsa (Sigma Aldrich, Nairobi) using standard procedures. The two thick smears were examined by two microscopists independently; one batch was examined at the field site (Butimba) and another batch at Bugando Medical Centre. The thin smears were used for identification of the malaria species. All discordant slides and 30 randomly selected slides were examined by the third expert for quality control. A slide was concluded to be negative when no parasites were observed after counting 200 white blood cells in different fields. The diagnosis of malaria using ParaHIT-f (Span Diagnostics Ltd, Surat, India, Lot 9624) was done according to manufacturer′s instruction. The paraHIT-f kits were stored below 40 0 C as recommended by manufacturer. The microscopists were blinded of RDT results, and positive smear results were used for initiating treatment according to Tanzania malaria treatment guidelines. In the analysis only positive slides by at least 2 readers were included. Data were analysed using SPSS version 11.5 (SPSS inc. Chicago). Sensitivity was calculated as true positive (TP)/ [TP+false negative (FN)], specificity as True negative (TN/ [(TN+false positive (FP)], Negative predictive value (NPV) as TN/(TN+FN) and Positive predictive value as TP/(TP+FP) (Neeru et al , 2005) There was a good agreement with only 5 slides showing discordant results between the first two readers. A total of 47 slides were positive by two readers and were included in the analysis. The prevalence of asexual Plasmodium falciparum parasitaemia was 5.7% (14) and 15.7% (47) by ParaHIT-f and microscopy, respectively. The asexual parasite density ranged from 40 to 300,000parasites/µl. The sensitivity, specificity, positive predictive value (PPV), negative predictive values (NPV) of ParaHIT-f using microscopy as gold standard were 29.8% ,98.8% , 82.4% and 88.3%, respectively [Table - 1]. There was a strong association between being positive by ParaHIT-f diagnostic test and parasitaemia (cut off point ≥1000parasites/µl ) (Fisher′s Exact test, P < 0.001), with ParaHIT-f picking only those with high parasite count. Microscopy detected malaria in patients with parasitaemia ranging from 40 to 300,000parasites/µl while ParaHIT-f detected only one patient with 160parasites/µl and others had parasitaemia above 600parasites/µl. Fever was the main presenting symptom reported by 95.3% (286) followed by cough 39%(117) and vomiting by 24.3%(73). Among children with fever only 46 (16.1%) had positive blood slide compared to only 1 (7.1%) of those children with no fever (Fisher′s Exact test, P =0.325). ParaHIT-f is a rapid, easily performed RDT with clear lines both in the control and in the test. Such a test and other RDTs are needed in the laboratories lacking trained microscopists in malaria endemic areas. RDTs are likely to facilitate early diagnosis and prompt treatment in endemic areas. The results of this study show that ParaHIT-f which is already available for use in Tanzania has low sensitivity of 29.8%. Similar results have been reported recently from Philippines (Belizario et al., 2005). The results however differ from what was reported in India where ParaHIT-f was reported to have higher sensitivity in areas with different epidemiological settings (Neeru et al., 2005). Reasons for the low sensitivity in this study were not investigated. However, it has been documented that when quality of RDTs is good deletion mutation or diversity in Pf HRP2 is likely to be the reason. Deletion mutation of Pf-HRP2 has been reported by Traole et al. (1997). Other RDTs targeting HRP2 have performed well in other parts of Tanzania (Mboera et al., 2006; Kamugisha et al., 2008). The difference in sensitivities of RDTs targeting Pf-HRP2 within the same country has been reported recently and is due to diversity in Pf-HRP2 gene (Baker et al., 2005; Natacha et al., 2008). Some repeats are associated with false negative results especially at low parasitaemia (Natacha et al., 2008). The difference could also be explained by storage conditions (WHO 2003, Mboera et al., 2006; McMorrow et al., 2008). However, in this study storage, procedures and transport were accordingly to manufactures instructions. Specificity of ParaHIT-f in this study was high 98.8% and the results were similar with other reports (Belizario et al., 2005; Neeru et al., 2005). In this study, ParaHIT-f also detected parasitaemia higher than 35,000parasites/µl contrary to what was reported by other studies (Neeru et al., 2005). The sensitivity of paraHIT-f was high at higher parasitaemia and there was a strong association between higher parasitaemia and being positive for ParaHIT-f ( P < 0.001). The same observation was reported by other studies; the main suggestions for their observations were the diversity in Pf-HRP2 gene, with certain repeats not able to be detected at parasitaemia less than 250parasites/µl. (McMorrow et al 2008; Natacha et al., 2008). In the present study, only 16.1% among children with fever had positive slides; this indicates the importance of reliable diagnostic tools to differentiate malaria and other causes of fever (Reyburn et al ., 2004). In conclusion, although ParaHIT-f highly specific in malaria diagnosis, it is less sensitive in the study area. The use of ParaHIT-f in Tanzania should therefore be revisited and countrywide studies are recommended to determine the sensitivity, specificity and other parameters of ParaHIT-f to ensure quality of the test.[10] References
Copyright 2009 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th09019t1.jpg] |
| |||||||||

{kind=link}