 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Journal of Health Research, Vol. 11, No. 3, July, 2009, pp. 149-153 Relative prevalence of methicilline resistant Staphylococcus aureus and its susceptibility pattern in Mulago Hospital, Kampala, Uganda J. Ojulong1*, T.P. Mwambu2, M. Joloba1, F. Bwanga1 and D.H. Kaddu-Mulindwa1 1Department
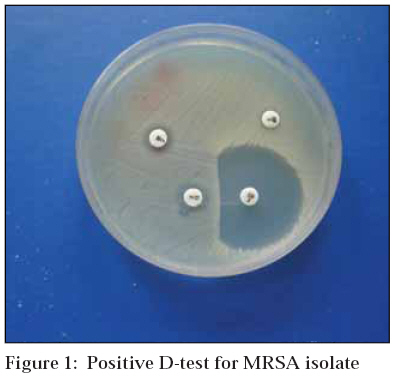
of Microbiology, Makerere University, Kampala, Uganda Received 16 May 2009 Code Number: th09026 Abstract Methicilline resistant Staphylococcus aureus (MRSA) strains are becoming increasingly multiresistant, and have recently developed resistance to vancomycin, which has been used successfully to treat MRSA for many years. In-vitro determination of resistance patterns of S. aureus is critical in terms of administering suitable antimicrobial treatments. The objective of this study was to determine the relative prevalence of MRSA among S. aureus isolates from surgical site infections and their antibiotic susceptibility pattern in Mulago Hospital, Kampala, Uganda. One hundred eighty eight pus swabs were collected from patients with surgical site infections. Swabs were inoculated for culture at the Microbiology Laboratory of the Faculty of Medicine, Makerere University. S. aurues isolates were identified using standard procedures and tested for oxacillin resistance according to methods of the National Committee for Clinical Laboratory Standards. Out of the 188 specimens, 54 (28.7%) grew S. aureus. Seventeen (31.5%) of the S. aureus isolates were confirmed as MRSA by PCR.Resistance rates of MRSA were 88.2% for trimethoprim-sulfamethoxazole, 88.2% for erythromycin, 58.8% for gentamycin, 70.6% for ciprofloxacin, and 88.2% for chloramphenicol. All isolates were found to be sensitive to vancomycin and clindamycin though the D-test was found to be positive in 82.4% of the isolates. In our region, although methicillin resistance increased in S. aureus strains, because of the unavailability and the high cost of alternative antibiotics, gentamycin is still suggested as an alternative for treatment of S. aureus infections. These results however indicate that vancomycin seemed to be the only antimicrobial agent effective against MRSA and it could be the drug of choice in treating multidrug resistant MRSA infection. Key words: Staphylococcus aureus, antibiotic, methicilline, resistance, susceptibility, Uganda Introduction Staphylococcus aureus is recognized as one of the most important bacterial pathogens seriously contributing to the problem of nosocomial and community acquired infections (Jan et al., 2002). Since the first isolation of methicillin-resistant S. aureus (MRSA) in the United Kingdom in 1961, increasing rates of methicillin resistance among S. aureus strains have been a cause for concern (Jevons, 1961; Gorwitz et al, 2006). MRSA is a major nosocomial pathogen that causes severe morbidity and mortality worldwide (Anjali & Daum, 999; Rodriguez & Khan, 1974). It spreads more readily than other strains once introduced into hospitals, and are often difficult to eradicate once established. In some countries MRSA make up to 75% of all S. aureus isolates in hospitals (Gorwitz et al., 2006; Kesah et al., 2003). Transmission of MRSA occurs primarily from colonized or infected patients or staff to other patients or staff, or vice versa. Among the resistant pathogens, MRSA is of great concern because of the importance in causing various clinical infections (Stefani & Varaldo, 2003; Kloos & Schleifer, 1986). Antimicrobial drug resistance has become a great public health problem worldwide (Aribas et al, 2001; Unlu & Unlu, 2001). As incidence of MRSA increased, the efficacies of penicillins and cephalosporins have waned. Essentially, many MRSA strains acquired resistance to both beta lactam and aminoglycosides. Therefore, it is necessary to know the MRSA prevalence and to choose suitable antibiotics with respect to their antimicrobial profiles for treating the infections (Aribas et al, 2001; Unlu & Unlu, 2001). The major challenge to controlling hospital infections has been due to emergence of multiple antibiotic resistant organisms among MRSA isolates. The knowledge of the pattern of antibiotic resistance among isolates is very important clinically and epidemiologically. The results of antimicrobial resistance patterns are of great concern due to the predominant bacterial isolates which are highly resistant to the commonly available antimicrobial agents. Lately, it has become increasingly reported in many countries that most hospital infections caused by MRSA have become multi-drug resistant (Aribas et al., 2001; Unlu & Unlu, 2001; Leclercq, 2002). For instance, MRSA accounts for nosocomial S. aureus infections in hospitals in the USA for up to 40% (Suntharam et al., 2001, Anjali & Daum, 1999; Rodriguez & Khan, 1974). While in Europe, prevalence is 2-50% (Chambers, 2001), studies in eight African Hospitals estimated the prevalence of MRSA to be 30% (Kesah et al., 2003). There are no published studies on the prevalence of MRSA strains and their resistance patterns against antibiotics in Uganda. The present study was undertaken to ascertain the relative prevalence of MRSA and its antibiotic susceptibility in Mulago National Hospital in Kampala, Uganda. The objectives were to determine the prevalence of MRSA and to investigate the resistance patterns of the isolated MRSA strains for various antibiotics. Materials and Methods Study site The study was conducted in Mulago National Hospital in Kampala, Uganda. It is the Uganda’s largest national referral, teaching and research hospital. It has an average inpatient of about 120,000 and attends to over 480,000 outpatients and delivers about 27,000 mothers per year. The hospital has a bed capacity of 1500, handling patients in and around Kampala Capital City. This study was performed to find the prevalence of MRSA infection from Surgical, Obstetrics and Gynaecology wards between February and May 2007. In this study, the isolation rate of coagulase positive Staphylococci was 28.7% (54/188) from pus swabs. Laboratory protocol Identification of S. aureus was confirmed by standard methods and susceptibility testing was performed by disc diffusion on Mueller-Hinton agar (Difco, USA) with 24-h incubation at 35°C. Interpretation criteria were those of the National Committee for Clinical Laboratory Standards (2003). Resistance to oxacillin was confirmed by agar screen method using an agar plate containing 6μg/ml of oxacillin and Mueller-Hinton agar supplemented with NaCl (4% w/v; 0.68 mol/L). Susceptibility of isolated MRSA strains to gentamycin (10 µg/disk), trimethoprim-sulphamethoxazole (25 µg/disk) erythromycin (15 µg/disk), clindamycin (2 µg/disk), chloramphenicol (30µg/disk), ciprofloxacin (5 µg/disk), and vancomycin (30 µg/disk) were tested as well as a D-test done. The clindamycin disk was placed at a standard distance of 15 mm from the erythromycin disc. The petri dish was then incubated at 35°C for 18 hours. "D zone “of inhibition was seen with an inducible strain of MRSA (Jorgensen et al., 2004). All antibiotic disks were obtained from (Liofilchem-Roseto-Italy). ATCC 25923 was used as the control strain for identification and susceptibility tests. Data analysis Statistical analysis was performed using a Chi-squared test and p-values less than 0.05 were considered statistically significant. The statistical analyses were performed by using STATA software. Ethical consideration A clearance from the Department Research Committee, Faculty of Medicine Research and Ethics Committee of the Makerere University, Uganda was sought. In addition, a written consent from participants was also obtained and the confidentiality of the information was guaranteed to the participants. Further still positive results were communicated to the Surgeon In-charge for management of patients. Results Fifty four (28.7%) isolates of S. aureus were analysed from 188 patients and 17(31.5%) were MRSA isolates which were studied. The most effective antibiotic against MRSA was vancomycin (Table 1). Resistance to trimethoprim/sulfamethoxazole, chloramphenicol and erythromycin were highest at 88.2%. Resistance to ciproflaxacin from the quinolone group and gentamycin was 70.6% and 58.8%, respectively. All strains were resistant to penicillin (resistance rate: 100%). Clindamycin sensitivity was found to be 100%, however, 82.4% of the isolates showed a positive D-test (Figure 1). Table1: Susceptibility pattern of methicilline resistant Staphylococcus areus isolates
When gentamycin and ciprofloxacin sensitivities to MRSA isolates were compared, 59% and 71% of the isolates were resistant, respectively. Discussion Many investigators have reported an increase in the incidence of MRSA during recent years, most of which originated from wounds (pus) (Mansouri & Khaleghi, 1997; Vidhani et al, 2001). Resistance to multiple antibiotics among the Staphylococci isolates in hospitals has been recognized as one of the major challenges in controlling hospital infections. The pattern of bacterial resistance is important for epidemiological and clinical purposes. The results of the antimicrobial resistance pattern give serious cause for concern because the predominant bacterial isolates were highly resistant to the commonly available antimicrobial agents. Recently, a substantial increase in the number of hospital infections due to MRSA has been reported in many countries (Leclercq, 2002; Kesah et al., 2003; Braun & Hassler, 2003). We also found a high rate of MRSA isolates i.e. 88.2% from the clinical specimens also showed multiple drug resistance. In our study, MRSA isolates were resistant to most antibiotics tested. We have observed in our study that resistance to different antibiotics among MRSA strains was quite high. Gentamycin, which was proposed to be an alternative therapy to MRSA infection, was found to be still better in this part of the world (52.6%). This is perhaps due to the different clonal expansion and drug pressure in the community. Another alternative to gentamycin treatment of MRSA infections would be clindamycin. However, due to cross resistance with erythromycin for patients who have ever been exposed to one drug, in this study, resistance was found to be high (82.4%). Erythromycin (a macrolide) and clindamycin (a lincosamide) represent two distinct classes of antimicrobial agents that inhibit protein synthesis by binding to the 50S ribosomal subunits of bacterial cells (Christine et al, 2005). In staphylococci, resistance to both of these antimicrobial agents can occur through methylation of their ribosomal target site. The target site modificationmechanism, also called macrolide-lincosamide-streptograminB resistance, results in resistance to erythromycin, clindamycin, and streptogramin B. Therefore S. aureus isolates that test as resistant to erythromycin and susceptible to clindamycin can still be resistant to clindamycin by an inducible or constitutive mechanism encoded by the erm gene by methylation of the 23S rRNA. Erythromycin has been found to be an effective inducer, yet clindamycin a weak inducer. Therefore, clinical failure may ensue when clindamycin therapy is instituted on patients who have taken or have been exposed to erythromycin (Christine et al, 2005). In this study all isolates of MRSA showed sensitivity to clindamycin. However, 82.4% of them were actually having inducible resistance to clindamycin. ** Recently, ina similar study in Tanzania clindamycin inducible resistance was observed in 61% of MRSA (Mshana et al., 2009). As high as 82% inducible clindamycin resistance has been reported in Kwa-Zulu Natal in South Africa (Shiitu & Lin, 2006). Since, complete eradication of MRSA may not be possible, control of transmission seems to be the appropriate goal. The efficacy of some controlling methods are widely recognized and recommended by most authors. The first and the most effective way among these are to avoid transmission through hand contamination by the person responsible for caring the infected patients. The use of broad-spectrum antibiotics for treating infections also increases the rate of MRSA and other resistant bacteria (Vidhani et al., 2001). Some patients can be treated with clindamycin, but inducible resistance may occur in some strains that appear susceptible in broth susceptibility tests. Therefore chemotherapy should be guided by sensitivity of the probable causative organism through accurate detection of MRSA by clinical laboratories as well as making a D-test a routine procedure. A further large study with a large sample should be carried out to find antibiotic susceptibility of MRSA in various hospitals in the East African region. References
Copyright 2009 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th09026f1.jpg] |
| |||||||||

{kind=link}