 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
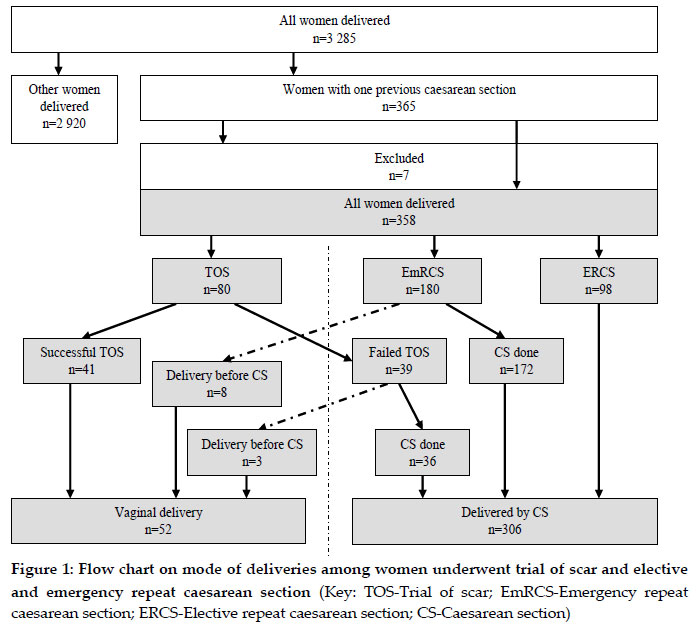
Tanzania Journal of Health Research, Vol. 12, No. 3, 2010 Pregnancy outcome after one previous caesarean section at a tertiary university teaching hospital in Tanzania ANDREA B. PEMBE* and MASHAVU K. OTHMAN Department of Obstetrics and Gynaecology, Muhimbili University of Health and Allied Sciences, P.O. Box 65117, Dar es Salaam, Tanzania * Correspondence: Dr. Andrea B. Pembe; Email: andreapembe@yahoo.co.uk Received 16 April 2010 Abstract: The aim of this study was to assess outcome of pregnancy in women with one previous caesarean section at Muhimbili National Hospital in Dar es Salaam, Tanzania. A cross sectional descriptive study was conducted at Muhimbili National Hospital (MNH) from 13th September 2006 - 2nd February 2007. All women with one previous caesarean section coming for delivery at MNH in that period were identified. Data on medical history, socio-demographic and obstetric characteristics, decision on mode of delivery, and pregnancy outcomes were collected. There were 3285 deliveries during the study period, out of which 365 (11%) women had one previous caesarean section. Almost half (48%) of the women with one previous caesarean section attended antenatal care in the dispensaries and health centres. Trial of scar was decided in 80 (21.9%) women. A total of 278 women had the decision for repeat caesarean section made on admission whereby 180 (64.4%) were for emergency caesarean section and 98 (35.6%) were for elective caesarean section. A total 52 women delivered vaginally, 44 after trial of the scar and eight among women decided for emergency repeat caesarean section on admission. The incidence of uterine rupture was 2% and perinatal mortality ratio was 55 per 1000 live birth. In conclusion, a significant proportion of women delivering at MNH had one previous caesarean section among which few underwent trial of scar. Half of the women attended antenatal care in the dispensaries and health centres. Women with previous caesarean section should be encouraged to attend hospitals providing comprehensive emergency obstetric care. The quality of intrapartum monitoring should be audited to improve maternal and newborn outcome. Key words: Caesarean section, trial of scar, high risk pregnancy, Tanzania IntroductionCaesarean section is one of the common surgical interventions to save lives of the mothers and/or the newborns. The rate of caesarean section has increased dramatically world wide over the past three decades (Bailit et al., 2004; Declercq et al., 2006). At Muhimbili National Hospital (MNH), a tertiary and university teaching hospital in Tanzania, there is steady increase in rate of caesarean section from 15.8% in 1999 to 31.8% in 2004 with nulliparous women more at risk (Muganyizi et al., 2008). Despite the gross increase in caesarean section rate there is still high perinatal mortality (Kidanto et al., 2006). Another study showed that repeat caesarean section is the second common indication for emergency caesarean section, the first being labour dystocia (Mdegela, 2006). Studies have shown that 30 - 80% of women with one previous lower segment caesarean section can achieve vaginal delivery when trial of scar is done (Landon et al., 2004; McMahon et al., 1996). Offering trial of scar and subsequent vaginal delivery can contribute to reduction of the rate of caesarean section. However, the risk of uterine rupture and other morbidities associated with failed trial of the scar, remain the major concern for many practitioners (McMahon et al., 1996). Few studies in Tanzania have reported delivery outcome of women with one previous caesarean section. The current study assessed obstetric outcome in women with one previous caesarean section delivering at MNH with the objective to determine the proportion of women undergoing trial of the scar, elective and emergency repeat caesarean section. Material and Methods Study setting and design This cross sectional descriptive study was conducted at Muhimbili National Hospital (MNH), which is the largest referral and teaching hospital in Tanzania. The hospital serves as a referral hospital for the city of Dar es Salaam and the neighbouring coastal region. The total number of deliveries is about 12000 per year. The hospital operates an open door policy where all pregnant women who come for delivery and have attended and not attended antenatal care at the hospital are received and managed irrespective of their clinical state. Women planned for elective caesarean section are admitted into the obstetric wards and sent to theatre directly for the operation. If labour starts before the scheduled date the decision for mode of delivery is reached by a team of doctors on duty. All women in labour are admitted in the labour ward. The nurse midwives in the admission room do general and abdominal examination, and then start a partograph. The initial vaginal examination and decision for trial of scar or emergency caesarean section is done by a registrar or more senior doctor. Those women decided for emergency caesarean section are sent to theatre for the operation. The study was conducted from 13th September 2006 - 2nd February 2007. Caesarean section There is an obstetric theatre with two rooms for operations. On average, 10 caesarean sections are performed each day. The transverse lower segment uterine incision is done to all mothers except when there is need for extending the incision into the upper segment or doing the incision in the upper segment (classical caesarean section). It is the policy that bilateral tubal ligation should be done to all cases of classical caesarean section. Closure of the uterine incision is done mostly in two layers using Catgut suture size one or two. Conduct of trial of scar Trial of scar at MNH is done to women with one previous caesarean section, vertex presentation and spontaneous onset of labour. It is started when labour is in active phase, defined as cervical dilatation of ≥3cm. Argumentation of labour is done by artificial rupture of membrane only when deemed necessary. Oxytocic drugs (syntocinon or prostaglandins) are not used for argumentation. Induction of labour is not done in a woman with one previous caesarean section. All women undergoing trial of scar, observation on vaginal bleeding, scar tenderness and colour of liquor is done every 30 minutes. Assessment of cervical dilatation, effacement and station of the presenting part is done every three to four hours. Maternal blood pressure and pulse record, and foetal heart sound record are taken every 30 minutes in early first stage of labour and 15 minutes in second stage of labour. Pinard’s stethoscope is used to monitor foetal heart sound. When foetal heart beats are difficult to hear by Pinard’s stethoscope, a portable doppler is used. There is no cardiotocographic (CTG) machine. The trial of scar is terminated if cervical dilatation graph shows any deviation to the right of the alert line, scar tenderness, unexplained maternal high pulse rate and fresh vaginal bleeding. Another reason for terminating trial of scar is foetal distress decided if there is fresh thick meconeum stained liquor, irregular foetal heart beats and/or heart beats of less than 120 or more than 160 in the absence of any obvious cause. The mother and the newborn are observed for at least 24 hours after vaginal delivery while those delivered by caesarean section are discharged on the third day if they have no complication. Data collection All women with one previous caesarean section delivered at the hospital with 28 weeks of gestation and above were identified on admission. The structured questionnaire was filled on admission and/or after the woman had delivered before discharge from the hospital depending on the patient’s convenience. The questionnaire included data on socio-demographic and obstetric characteristics, medical history and outcome of index pregnancy. The health facility the woman attended antenatal care was ascertained on their antenatal card. For those referred and attended the MNH antenatal clinic were taken as MNH attendees confirmed by the hospital registration number on the front page. The records from obstetric theatre, labour ward and postnatal wards were used to ensure all information was collected. Data analysisStatistical analysis was conducted using SPSS 14.0 computer programme. Frequency distribution and measure of location were used to summarize data. Ethical considerationEthical clearance was obtained from the Senate, Research and Publication Committee of Muhimbili University of Health and Allied Sciences. The permission to conduct the study was given by the Executive Director of MNH. Informed consent was obtained from all women with one previous caesarean section, no one declined to participate. ResultsA total of 3285 women delivered at MNH during the study period, out of which 365 (11%) had one previous caesarean section. Seven women were excluded from the study; three had no foetal hearts on admission, one had abdominal pregnancy and other three their case notes were incomplete. Eighty out of 358 (22%) women underwent a trial of scar while 98 (27%) were decided to undergo elective repeat caesarean section and 180 (50%) emergency repeat caesarean section. Among the 80 women who underwent trial of the scar, 44 (55%) delivered vaginally and 8 delivered vaginally while waiting for emergency repeat caesarean section, giving a total of 52 (15%) women with one previous caesarean section delivering vaginally. Among 44 women who delivered vaginally after trial of the scar, three delivered while waiting for caesarean section after decision for failed trial of the scar was declared (Figure 1). Out of 358 women, 356 (99%) attended antenatal care. One hundred and seventy two (48%) women attended dispensaries and health centres. The majority, 226 (63%) had no decisions for suggested mode of delivery indicated on their antenatal cards. This was more common among women who attended antenatal care at dispensaries and health centres. At MNH where most women had decisions for mode of delivery indicated in the antenatal card almost two thirds were suggested to undergo elective repeat caesarean section (Table 1). Table 1: Facilities women attended antenatal care and decision for mode of delivery indicated on the antenatal card
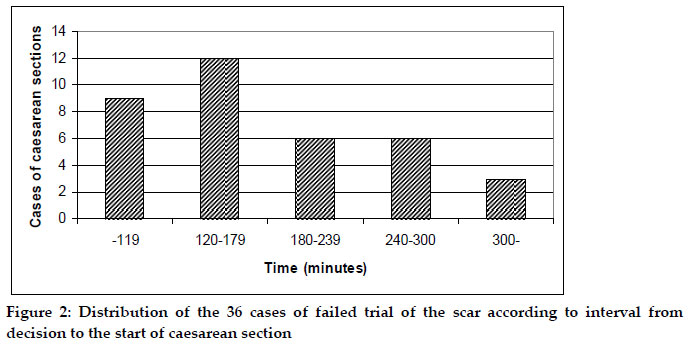
aTwo women did not attend antenatal care Among women who had trial of the scar, labour dystocia accounted for 61% as a reason for failed trial of scar. Other reasons were impending rupture 10 (27.8%), foetal distress 3 (8.3%) and one case the reason was not indicated. The median time from decision of failed trial of the scar to start of caesarean section delivery was 141 minutes (range: 70- 444 minutes) (Figure 2). Labour dystocia was the commonest indication of emergency repeat caesarean section. Previous history of labour dystocia leading to caesarean section was as well leading indication in elective repeat caesarean section. A significant number of women were delivered by emergency or elective repeat caesarean section due to pregnancy induced hypertension or eclampsia (Table 2). Table 2: Indication of emergency and elective repeat caesarean sections among women not underwent trial of scar
aHistory of labour dystocia and BOH in the previous
pregnancies in the elective caesarean section. There were seven cases of uterine rupture among 358 women who had one previous caesarean section, giving the incidence of 2%. All were women decided for emergency repeat caesarean section; two women had tenderness on the scar without labour and the remaining five none was suspected to have ruptured uterus before the operation. One of the seven cases of uterine rupture underwent hysterectomy. There was one maternal death. This was one of the cases of ruptured uterus and woman died 24 hours after the operation. Severe and mild birth asphyxia was observed in six (1.7%) and 18 (5%) newborns respectively. Eighteen newborns died during delivery and within 24 hours of delivery giving the perinatal mortality ratio of 56 per 1000 live births. Perinatal mortality ratio per 1000 deliveries was 100 among women who underwent trial of scar, 44 among women underwent emergency repeat caesarean section and 20 among those underwent elective repeat caesarean section (Table 3). Table 3: Number (%) of foetal outcome according to the mode of delivery
Key: EmRCS-Emergency repeat caesarean section; ERCS-Elective repeat caesarean section; Discussion In this study we found women with one previous caesarean section constitute 11% of all deliveries at MNH. Among these women almost half has attended antenatal care in dispensaries and health centres. Less than a quarter of the women underwent trial of scar, a quarter had elective repeat caesarean section and the remaining half had emergency repeat caesarean section. The incidence of ruptured uterus was 2% and the perinatal mortality ratio was 56 per 1000 live birth. The high proportion of women with one previous caesarean section at MNH could be explained by the fact that MNH is a referral hospital and not all three municipal hospitals in the city provide 24-hour comprehensive emergency obstetric care services (Nyamtema et al., 2008); this necessitates dispensaries and health centres to refer these women directly to MNH. Almost half of the women had attended antenatal care in the dispensaries and health centres. These facilities are primary level of care which do not provide comprehensive emergency obstetric care. The Reproductive and Child Health card number 4 (RCH-4) indicates that all women with previous caesarean section should be referred to health centre or hospital for further assessment or counselling on the day they book for antenatal care. It further explains that the provider should advice the woman to seek delivery care at the health centre or hospital (MoHSW, 2006). Most dispensaries and health centres in Tanzania provide normal delivery services, therefore referral from dispensaries to health centres do not add any advantage to the women. Early referral during antenatal care to hospitals which provide comprehensive emergency obstetric care can help providers in the hospitals to plan in advance mode of delivery especially women with malpresentation or contracted pelvis who require elective caesarean sections. Less than a quarter of the women had a chance to undergo trial of the scar. Even if all women underwent trial of scar would have delivered vaginally, still the proportion is small to contribute to overall reduction of caesarean section rate. Studies elsewhere have demonstrated a comparable higher proportion of women with previous caesarean section are allowed to undergo trial of scar (Aisien & Oronsaye, 2004; McMahon et al., 1996). The small proportion of women with one previous caesarean section undergoing trial of scar at MHN can be speculated as a result of the pressure put on doctors as many women admitted have not been seen by the doctors before and are in labour. Furthermore doctors and women have pressure of getting babies with good apgar scores, and not repeating previously experience of bad outcome. In other parts of the world, the proportion of women with one previous caesarean section undergoing trial of scar is reduced not only due to fear of complication but litigation. The obstetrician will rarely be blamed for doing a caesarean section, while may be sued for not having done it (Fuglenes et al., 2009). Among women who underwent trial of scar more than half successfully delivered vaginally. This success rate is lower compared to other studies (Durnwald & Mercer, 2004; Landon et al., 2004; McMahon et al., 1996; van Roosmalen, 1991). The lower success rate in our study may be due to differences in choosing eligible cases or premature decision for failed trial of scar. A study in a Southern Africa district hospital reported that delivery in subsequent pregnancy is not influenced by indication of primary caesarean section being recurrent or nonrecurrent (van Bogaert, 2004). However, other studies have shown that vaginal delivery is higher for those with nonrecurrent indication in the primary caesarean section (Butt & Akhtar, 2005; Cecatti et al., 2005). The incidence of 2% of ruptured uterus in women with one previous caesarean section in this study is slightly higher than other studies which show the incidence to be between 0.2% and 1.5% (Aisien & Oronsaye, 2004; McMahon et al., 1996). All ruptured uterus in our study occurred in women decided for emergency repeat caesarean section. Majority of the women decided to undergo emergency repeat caesarean section were admitted after having laboured outside the hospital. Uterine rupture with its consequence of morbidity and mortality to the mother and foetus is the most threatening risk of allowing trial of scar. The overall perinatal mortality ratio of 56 per 1000 live birth is high compared to other studies (Aisien & Oronsaye, 2004; Butt & Akhtar, 2005). A high proportion of perinatal deaths in our study occurred in women who underwent trial of scar. A study in Peshawar reported higher perinatal deaths among women decided for emergency repeat caesarean section (Butt & Akhtar, 2005). Our results may be reflecting on the referral of women to the facilities providing comprehensive emergency obstetric care and the quality of monitoring of labour during the trial of the scar and any woman in labour. Furthermore, taking into consideration majority of the women had caesarean section two hours after decision was made indicates low quality of services for obstetric emergencies at the hospital. There is need to audit quality of care in all women in labour, women undergoing trial of the scar, and decision for emergency caesarean caesareans. Having two stillbirth babies in the elective repeat caesarean section show that in our centre even caesarean section is not very safe either for the mother or the baby. We are still convinced that trial of scar in patients with one previous caesarean section is almost always safe in institutions which have good quality of care and should be provide in health facilities capable to provide comprehensive emergency obstetric care. In conclusion, there is significant proportion of women delivering at MNH with one previous caesarean section and very few are given chance to attempt vaginal delivery. Half of the women had attended antenatal care in the dispensaries and health centres to be seen at MNH when in labour. To reduce perinatal morbidity and mortality, it is proposed that all women with one previous caesarean section should be encouraged to attend antenatal care in hospitals providing comprehensive emergency obstetric care and doctors in these hospitals should be encouraged to offer trial of scar. Studies are needed on clinical audit of cases of one previous caesarean section and all cases of primary caesarean section in the hospital. AcknowledgementsMs Blandina Nyoni of the Muhimbili National Hospital is thanked for assisting in data collection. The authors are grateful to Mr. Charles K. Makwaya for his assistance in data management. References
Copyright 2010 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th10025f2.jpg] [th10025f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}