 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Journal of Health Research, Vol. 12, No. 4, Oct, 2010, pp. 1-9 Motorcycle injuries as an emerging public health problem in Mwanza City, north-western Tanzania Phillipo L. Chalya*, Joseph B. Mabula, Isidor H. Ngayomela, Emmanuel S. Kanumba, Alphonce B. Chandika, Godfrey Giiti, Brian Mawala, Darius Balamuka Department of
Surgery, Weill- Bugando University College of Health Sciences, Mwanza, Tanzania Received 15
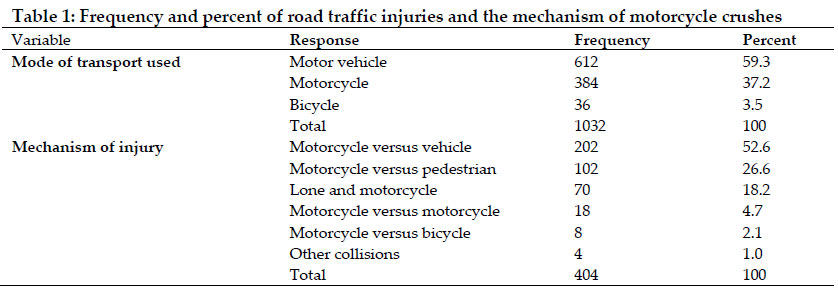
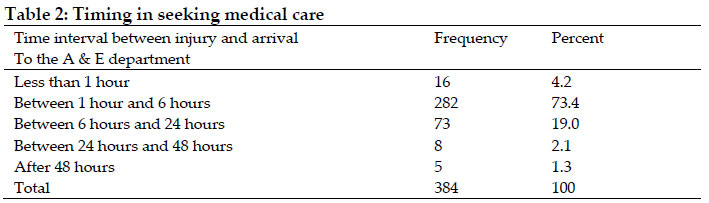
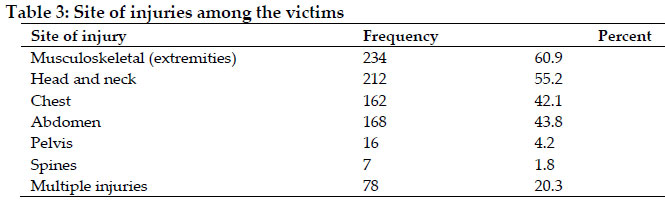
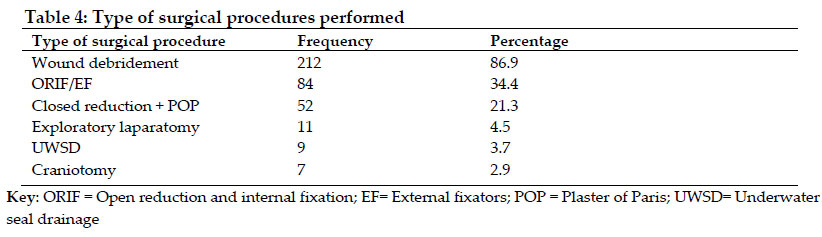
February 2010 Code Number: th10029 Abstract Motorcycle injuries constitute a major but neglected emerging public health problem in developing countries and are a common cause of road traffic injuries. The aim of this study was to establish the prevalence, injury pattern and treatment outcome of motorcycle injuries among patients presenting to Bugando Medical Centre in Mwanza, Tanzania, between March 2009 and February 2010. Data was collected using a pre-tested, coded questionnaire. A total of 384 motorcycle injury patients were studied constituting 37.2% of all road traffic injuries. Over two-thirds (69.5%) of the patients were males (Male: Female ratio = 2.3:1). The mean age of the patients was 25.7 years (range: 4-87 years). The majority of patients were businessmen and students accounting for 68.8% and 42.2%, respectively. Motorcyclists accounted for the majority of motorcycle injury patients (212, 55.2%), followed by passengers (130. 33.9%) and pedestrians (42, 10.9%). Helmet use was recorded in 87 patients (22.7%). Most patients (352; 91.7%) sustained blunt injuries. Musculoskeletal (extremities) and head injuries were the most common body region injured affecting 234 (60.9%) and 212 (55.2%) patients, respectively. The majority of patients (244; 63.5%) were treated surgically. Wound debridement was the most common (86.9%) procedure performed. The overall mean length of hospital stay (LOS) was 19.23 days (range= 1-120 days). The LOS for non-survivors was 5.6 days (range= 1- 25 days). Patients with major trauma (ISS > 16), severe head injury (GCS 3-8) and those with long bone fractures stayed longer in the hospital and this was significant (P-value <0.001). Mortality rate was 16.7% (64 deaths). Age of the patient, non-helmeted patients, major trauma (ISS > 16), admission systolic blood pressure <90mmHg, severe head injury (GCS <9), need for intensive care unit admission and need for ventilatory support significantly influenced mortality (P-value < 0.001). Motorcycle injuries constitute a major but neglected emerging public health problem in Mwanza City and continue to be one of the most common cause or agent of road traffic injuries. The morbidity and mortality can be mitigated by encouraging use of protective gear like helmets and encouraging enforcement of traffic laws. Key words: motorcycle injuries; prevalence, treatment outcome, injury pattern, Tanzania Motorcycle injuries constitute a major but neglected emerging public health problem in developing countries and contribute significantly to the overall road traffic injuries (Peden et al, 2002). Motorcycle injuries are among the leading causes of disability and deaths and the main victims are the motorcyclists, passengers and pedestrians in their young reproductive age group (Peden, 2004; Solagrebu et al., 2006). The problem is increasing at a fast rate in developing countries due to rapid motorization and other factors (Galukande et al, 2009).The injuries related to motorcycles contribute significantly to the number of road traffic injuries in Mwanza city, taking out significant resources including consumables and the health worker time. Motorcycle users are vulnerable on the road and represent an important group to target for reducing road traffic injuries (Solagrebu et al, 2006). Even in developed countries with low morbidity and mortality rates from motorcycle injuries, the risk of dying from a motorcycle crash is 20 times higher than from a motor vehicle crash (Peden, 2004; Solagrebu et al, 2006). The motorcyclists tend to over-speed and over load their motorcycles for quick returns. It is because of that recklessness, indiscipline and lack of respect for other road users by the motorcyclists who are mainly youths, are the major cause of road related injuries. The majority of the motorcyclists don’t wear any protective gear, hence aggravating the risks of getting severe head injuries (Naddumba, 2004). The motorcycle, commonly called “bodaboda” in Uganda and Kenya (Naddumba, 2004, Galukande et al., 2009) and ‘‘okada’’ in Nigeria (Oluwadiya et al., 2004; Solagrebu et al., 2006), has recently become increasingly popular in Tanzania as a means of commercial transport but their operation is characterized by non-helmet use by riders and their passengers, passenger overload, lack of certified driver training and valid licensing, over speed and reckless driving, poor regulation and law enforcement and possible use of alcohol and drugs (Museru & Leshabari, 2002). The popularity of this mode of transport in Tanzania can be due to the following reasons; they are a quick means of transport especially for short distances in cities and towns, they are efficient in mitigating traffic jam delays in the cities and they are available throughout the day and night hours. The negative side of motorcycle as a means of transport is the risk of injury as reported in other studies (Naddumba, 2004; Galukande et al., 2009) and they constitute a major public problem in major cities in developing countries like Tanzania (Museru & Leshabari, 2002). Despite the burden of the problem in Mwanza City, motorcycle injuries have not received the attention they deserve partly because of lack of local data, and the public policy responses to this epidemic have been muted at regional and national level. Since the majority of motorcycle injuries are preventable, a clearer understanding of the magnitude, contributing factors, injury patterns and outcome of these patients is essential for establishment of prevention strategies as well as treatment protocols (Solagrebu et al., 2006; Alicioglu et al., 2008). The objective of this study therefore, was to determine, the prevalence, injury patterns and outcome of treatment of motorcycle injuries among patients attending Bugando Medical Centre in Mwanza, Tanzania. The study provides basis for establishment of prevention strategies as well as treatment protocols. Materials and Methods Study Site and Patients This was a descriptive cross-sectional study of patients with motorcycle injuries of all age groups and gender presenting to the Accident and Emergency (A&E) of Bugando Medical Centre between March 2009 and February 2010. Bugando Medical Centre (latitude 2.52680 S; longitude 32.9062 E) is a 1000-bed, consultant and teaching hospital located in Mwanza, along the shores of Lake Victoria in north-western Tanzania. Trauma patients are first resuscitated and managed at the A&E Department according to the Advanced Trauma Life Support (ATLS) principles and then admitted to the admitting surgical firm. All recruited patients were first resuscitated in the A&E Department and were then taken into the surgical wards or the intensive care unit (ICU) from where necessary investigations were completed and further treatment was instituted. Variables studied included age,sex, occupation, injury host status (rider, passenger or pedestrian), mechanism of injury (motorcycle versus motorcycle, motorcycle versus other vehicle, motorcycle versus pedestrian, lone and motorcycle, and other collisions), prehospital transportation (relative, police and bystanders), injury arrival interval, helmet use, trauma scores (Injury Severity Score, Revised Trauma Score, Paediatric Trauma Score), body region injured and radiological findings. Outcome measures were mortality and length of hospital stay. All patients were followed up till discharged or death. This information was collected using a pre-tested questionnaire. Data analysis Data was analyzed using SPSS computer software version 11.5. A p-value of 0.05 was considered statistically significant. Ethical considerations All patients who met the inclusion criteria were, after informed consent to participate in the study, consecutively enrolled into the study. Patients who failed to give proper information and those who had no relative to consent for the study were excluded from the study. Ethical approval to conduct the study was obtained from the Weill Bugando University College of Health Sciences/Bugando Medical Centre Joint institutional Ethic Review Committee before the commencement of the study. Results A total of 1032 road traffic injuries were reported during the study period. Motorcycle traffic injuries accounted for 37.2% of all traffic injuries. Of the total patients, 267 (69.5%) were males and 117 (30.5%) were females (M:F ratio = 2.3:1). The patients’ ages ranged from 4 to 87 years with a mean of 30.7 years and a peak incidence of 21-30 years. The majority of patients (302; 78.6%) had primary or no formal education. In this study, the majority of the patients were businessmen (68.8%), followed by students (42.2%), public servants (31.5%), children (29.9%) and peasants (22.9%). Motorcycle versus vehicle accounted for the majority of types of crushes (Table 1). Motorcyclists accounted for the majority of motorcycle injury patients (212, 55.2%), followed by passengers (130. 33.9%) and pedestrians (42, 10.9%). Helmet use was recorded in 87 patients (22.7%). The majority crushed into moving vehicles. Regarding the time of the accident, 284 (73.9%) accidents occurred during the day, 92 (23.9%) at night and in 8 (2.2%), the time was not specified. The majority of patients arrived at the hospital between 1 and 6 hours (282, 73.4%). None of our patients had pre-hospital care. The majority of them were brought in by relatives and Good Samaritan in 55.7% (214 patients). One hundred and sixty-eight (48.8%) patients were brought in by police and only two (0.5%) patients were brought in by ambulance. The waiting time (i.e. time interval taken from reception at the A & E Department and reception of treatment) ranged from 10 minutes to six hours (mean= 2 hours). The majority of patients (321; 83.6%) were attended to within 1-2 hours of arrival to the A & E department (Table 2). The vast majority of patients (352; 91.7%) sustained blunt injuries and the remaining eight (8.3%) sustained either penetrating or both. Musculoskeletal (extremities) and the head were the most common body region injured affecting 234 (60.9%) and 212 (55.2%) patients, respectively (Table 3). Musculoskeletal injuries included soft tissue injuries (bruises, laceration, abrasion and contusions) in 197 injuries (84.2%) and fractures in 182 injuries (77.8%). Musculoskeletal injuries commonly affected the lower limbs. One hundred and five (54.2%) patients had mild head injuries (Glasgow Coma Scale [GCS]: 13-15), 75 (35.4%) had moderate head injuries (GCS: 9-12), and 22(10.4%) had severe head injuries (GCS: >8). No patient who had helmet at the time of accident sustained head injury. The most common complaints were loss of consciousness, headache and confusion. Skull X-ray performed in 67 cases showed fractures in eight cases only (six mild head injury and two moderate head injury), and was normal in all cases. Computed tomography (CT) scan of the brain performed in 36 cases revealed positive findings in 15 cases; most common findings were cerebral oedema (9 cases), linear fracture (8 cases), and extradural haematoma (5 cases). All patients with severe head injuries did not wear helmet at the time of injury. Abdominal injuries ranked third and all except one patient who sustained penetrating abdominal injury were blunt injuries. Four patients had ruptured spleen, one patient had liver laceration and one patient had retroperitoneal haematoma and urethral injury, one patient who had penetrating abdominal injury had gastric and transverse colon injury. The other patients had blunt injuries without visceral injury. Chest trauma was recorded in 162 patients (40.1%) and they were all blunt injuries including rib fractures (in 9 patients), hemothorax (in 7cases) and lung contusion (in 3 patients). Sixteen patients had pelvic injuries. Of these, 12 patients had minor pelvic injuries and the remaining 4 patients had major pelvic injuries. Spinal injuries were noted in seven patients (2 cases cervical, 4 cases lumbar and 1 case lumbosacral injuries). Two patients had paraplegia and one patient had quadriplegia. Injury severity score (ISS) was calculated in 78 cases. The overall ISS ranged from 1– 45 (mean 12.8). The mean ISS for motorcyclists was 13.9 (range 1 – 26), passengers 11.8 (range 1 – 28) and pedestrians 10.6 (range 1– 40). The majority of patients (76.4%) sustained mild to moderate injuries (ISS < 16). Severe injuries, ISS >16, occurred only in 23.6 % of cases, with a mean ISS of 21.1 (range 16–45). The majority of patients (298; 77.6%) were admitted in the general surgical wards. Twenty-four (6.3%) patients had an overnight stay at the Accident & Emergency Department and then discharged. Sixty-two (16.1%) patients were admitted in the ICU; of these, 42 (67.7%) necessitated ventilatory support. The majority of patients (244; 63.5%) were treated surgically. Wound debridement was the most common procedure performed in 212 (86.9%) patients (Table 4) The overall length of hospital stay ranged from 1 day to 120 days (mean 19.23 days). The LOS for non-survivors ranged from 1 day to 25 days (mean 5.6 days). The length of ICU stay ranged from 1 to 28 days (mean=7.8 days). Patients with major trauma (ISS >16), severe head injury (GCS 3-8) and those with long bone fractures stayed longer in the hospital and this was significant (P-value <0.001). In this study, sixty-four patients died, giving a mortality rate of 16.7%. Age of the patient, non-helmeted patients, major trauma (ISS >16), admission SBP <90mmHg, severe head injury (GCS <9), need for ICU admission and need for ventilatory support, significantly influenced mortality (P< 0.001). Discussion In recent years, there has been a significant increase in the number of motorcycle accidents in Mwanza City in parallel with increasing use of motorcycles as a commercial means of transport (Mwanza Traffic Police Injury Statistics & Tanzania Revenue Authority, 2008/2009, unpubl.). Injuries related to motorcycle contribute significantly to the number road traffic injuries seen at Bugando Medical Centre, taking out a significant number of lives and resources including consumables and the health worker time. However, despite this burden, the public policy responses to this problem have been muted, probably because of lack of local data regarding the problem. The prevalence of motorcycle injuries of 37.2% is higher than that recorded in Kampala, Uganda (25%) (Naddumba, 2004) and Benin City in Nigeria (18%) (Nzegwu et al., 2008), but it is lower than that reported in another studies in Nigeria (Okeniyi et al., 2005) and India (Fitzharris et al., 2009) where the prevalence of motorcycle injuries was reported to be 50.2% and 56.1% respectively. Aniekan & Sydney (2005) in Nigeria also reported a high prevalence of 47.3%. These differences in prevalence reflect differences in risk factors for motorcycle accidents between the study settings. The young male preponderance in the present study agrees with findings reported elsewhere (Naddumba, 2004; Andrews et al., 1999; Okeniyi et al., 2005; Solagrebu et al., 2006; Galukande et al., 2009). High occurrences of motorcycles accidents among this group have been attributed to a wide range of activities engaged in by this class of people. They are more likely to have reasons to move from one place to another. They represent the active group that partake in high risk-taking activities such as recklessness riding, over-speeding and overloading their motorcycles, riding under the influence of alcohol and riding without wearing any protective gears. Males are more often exposed to traffic as drivers; they travel longer distances to work and are more often involved in use of automobile as leisure activities (Akinpelu et al., 2007). Motorcycle riding in this area is almost exclusively men, most of whom do it for commercial purposes. Businessmen and students were the most injured because of the rush through heavy traffic to get to their businesses and to the school. Similar observation was noted by Naddumba (2002) in Kampala, Uganda. Solagrebu et al. (2006) also reported similar observation in Nigeria. Businessmen are often involved in buying and selling which necessitates movement from one place to another. This often involves travelling with good purchased, and in order to maximize profits, they usually opt for the cheapest means of transport available such as motorcycles. Students are usually involved in motorcycle accidents as they rush through heavy traffic to and from their schools. These school-age group children are usually very active and are often less supervised than pre-school age children. Coupled with the paucity of boarding school facilities for children of their age as well as of school buses, schoolchildren have to walk varying distances to and from school. This was the case in the vast majority of children knocked down in this study. As students formed one of the largest group of motorcycle injury victims, an improved school transportation system that obviates students’ need for the motorcycle may reduce the incidence of motorcycle injuries. Motorcycle use is becoming popular in Tanzania as it has become a cheaper and easier means of transportation in most cities. Motorcyclists are usually vulnerable to motorcycle accidents in that the majority of them are driving while intoxicated and exceeding the speed limit. Alcohol usage causes carelessness and loss of concentration as well as over speeding and neglecting to use safety equipment such as helmet. In the present study, motorcyclist constituted the majority of motorcycle injury victims. This is in agreement with other findings reported elsewhere (Solagrebu et al., 2006; Nzegwu et al., 2008), but in contrast with Naddumba (2006) and Okeniyi et al. (2005) who reported pedestrians as the majority of victims affected. In most cities in developing countries pedestrians signs are either absent or not observed by pedestrians or drivers and this has been responsible for high rate of fatality among pedestrians. Motorcycle helmets have been reported in literature to reduce the risk of death and head injuries (Offner et al., 1992; Brandt et al., 2002; Keng, 2005). However, studies have shown that helmet use in developing countries is low (Odelowo, 1994; Oluwadiya et al., 2004). In the present study, helmet use was recorded in 22.7% which is higher than that reported in Uganda (Galukande et al., 2009). Nzegwu et al. (2008) in Benin City, Nigeria reported that all motorcyclists and their passengers did not usehelmets. The same trend of non-usage of crash helmet was demonstrated in Lagos (Falope, 1991) and in Kampala (Andrews et al., 1999). Catherine et al. (2008) in Victoria reported high incidence of helmet use in 53% of patients. These differences in the rate of helmet use reflect differences in awareness of factors contributing to crush occurrence and injury severity related to motorcycle accidents between these countries and poor enforcement of traffic laws. The differences in helmet use may also imply different attitudes to helmet wearing between these countries. The reasons for non-compliance were not specifically studied but may include the cost of the helmet, ignorance, a cultural disposition toward lawlessness, fatalism, insufficient educational campaigns, and/or recreational drug use, which has been associated with non-compliance (Sauter et al., 2005).Other arguments that have been advanced in opposition to helmet use include impaired rider vision, attenuation of critical traffic sounds, rider fatigue and increased neck injuries in the event of a collision (Solagrebu et al., 2006; Liu et al., 2008; Ivor et al., 2009). However, none of these alleged disadvantages have been supported by evidence. The finding that most of injuries in the present study occurred during the day agrees with that of Naddumba (2006) in Uganda and Twagirayezu et al. (2008) in Rwanda. Increased rate of injuries during the day can be explained by increased traffic density as well as increased human activities in the city during the day time. Knowing the time of injury in trauma patient is important for prevention strategies. In agreement with another study in Nigeria by Solagrebu et al (2006), the majority of patients in this study arrived at the hospital relatively late. Despite the finding that the time interval between arrival and reception of initial treatment at the A & E Department did not influence the outcome of these patients, the delay in seeking medical care is likely to contribute significantly to high morbidity and mortality among trauma patients. Waiting time in emergency departments may be attributable to many factors and may stretch up to three hours before completion of all necessary procedures, even in developed countries (Silverston, 1985). This study found that the majority of the patients were attended to within 1-2 hours of arrival at the A & E Department. Lambe et al. (2003) reported a lower mean waiting time of 56 minutes in California, USA. Review of emergency department administration has been demonstrated to improve efficiency in care delivery (Havili et al., 1996). A waiting time of 30 minutes for a general outpatient clinic is considered reasonable but should be even shorter for emergency visits (Huang, 1994, Kyriacou et al, 1999). The prehospital care of trauma patient has been reported to be the most important factor in determining the ultimate outcome after the injury. None of our patients had pre-hospital care; as a result the majority of them were brought in by relatives, Good Samaritan and police who are not trained on how to take care of patients during transportation. This observation is common to many other developing countries. The lack of advanced pre-hospital care and ineffective ambulance system for transportation of patients to hospitals are major challenges in providing care for trauma patients in developing countries. In the present study, the collision between motorcycle and motor vehicle was the most common mechanism of injury followed by collision between motorcycle and pedestrians. Similar trend was also reported by Solagrebu et al. (2006) and Twagirayezu et al. (2008). The motorcycle-vehicle and motorcycle-pedestrian collisions occur commonly because the majority of the riders often ignore safety measures, making them more vulnerable to accidents with other motorized vehicles (Oluwadiya et al., 2004; Solagrebu et al., 2006). In addition, the absence of pedestrian walkways in most of the roads in Tanzania has increased the vulnerability of pedestrians to all motorized vehicles. Previous studies have shown that musculoskeletal and head injuries are the commonest causes of morbidity and mortality in motorcycle injuries (Solagrebu et al., 2006; Naddumba, 2006; Alicioglu et al., 2008; Galukande et al., 2009), attributing the latter to the low use of motorcycle helmets in our study; a situation seen in other developing countries. In the present study, no patient who was helmeted at the time of injury sustained head injury reflecting its importance in prevention of head injuries among motorcycle injury patients. The length of hospital stay (LOS) has been reported to be an important measure of morbidity among trauma patients. Prolonged hospitalization is associated with an unacceptable burden on resources for health and undermines the productive capacity of the population through time lost during hospitalization and disability. The figures for the overall mean LOS in the present study were higher than that reported by Alicioglu et al. (2008). Prolonged LOS in our study is attributable to presence of major trauma patients, severe head injuries and large number of patients with long bone fractures. The overall mortality rate in this study was higher than that reported elsewhere for motorcyclists (Alicioglu et al., 2008). Factors responsible for high mortality in our study included extremes of age, non-helmeted patients, major trauma, admission SBP < 90mmHg, severe head injury, need for ICU admission and need for ventilatory support. In conclusion, motorcycle injuries constitute a major but neglected emerging public health problem in Mwanza City. The young adult males in their reproductive and productive age group are commonly affected. Businessman and students are the largest groups of motorcycle injury victims. Limb and head injuries are the most common types of injury sustained predisposing these patients to prolonged hospitalization and mortality. Since the majority of motorcycle injuries are preventable, the following safety measures as suggested by Naddumba (2006) in Kampala, Uganda are highly recommended: (i) protective gear to include a helmet, eye and face protection, long pants, gloves, boots and a durable long-sleeved jacket; (ii) restriction of alcohol consumption before operating a motorcycle; (iii) strict enforcement of traffic laws and regulations; (iv) headlights to be kept on all the time during motorcycle riding; and (v) all motorcycle riders' should undertake course before being licensed as motorcyclists. Acknowledgements The authors would like to thank the members of staff of Surgical Department for their invaluable contributions in the preparation of this manuscript. References
Copyright 2010 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th10029t2.jpg] [th10029t3.jpg] [th10029t1.jpg] [th10029t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}