 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Journal of Health Research, Vol. 12, No. 4, Oct, 2010, pp. 237-242 Prevalence of congenital malaria among neonates at Morogoro Regional Hospital, Morogoro, Tanzania Theobald C.E. Mosha, Devote Ntarukimana, Matilda John Department of Food Science and Nutrition, Sokoine University of Agriculture, P.O. Box 3109, Morogoro, Tanzania Received: 25
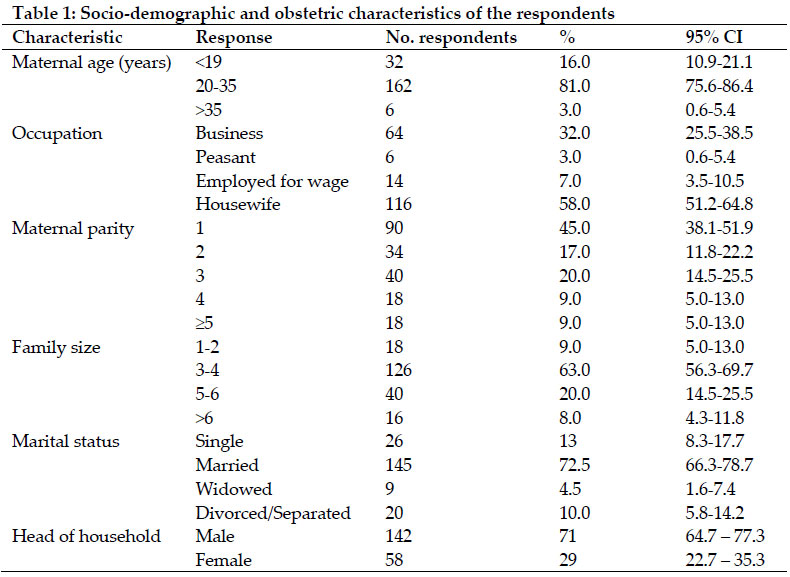
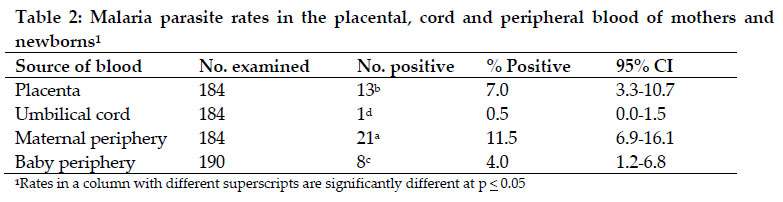
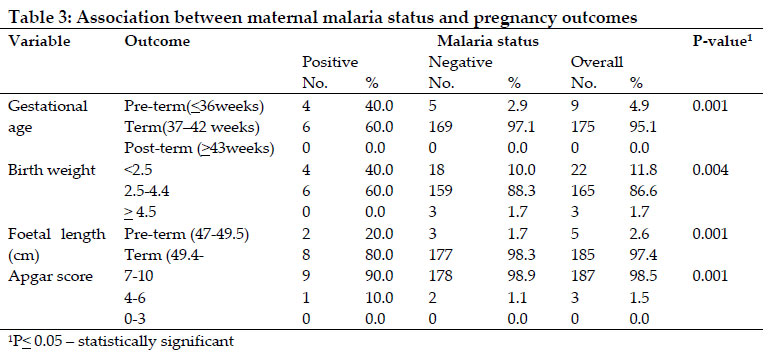
February 2010 Code Number: th10033 Abstract Congenital malaria is increasingly reported among babies born to mothers living in malaria endemic areas. The aim of this study was to determine the prevalence of congenital malaria among newborn babies delivered at Morogoro Regional Hospital, Tanzania. A cross-sectional study was conducted among 200 pregnant women attending delivery services at the hospital. Socio-demographic and obstetric information of the mothers was also collected. Samples of the placental, cord and peripheral blood smears of mothers and babies were stained with Giemsa and examined for malaria parasites. Plasmodiun falciparum was the dominant malaria parasite species. The prevalence of congenital malaria among newly born babies was 4.0% (95% CI, 1.2–6.8%). Prevalence of placental parasitaemia was 7.0% (95% CI, 3.3–10.7%), while prevalence of cord parasitaemia was 0.5% (95% CI, 0.0–1.5%). The prevalence of malaria among the mothers at delivery was 11.5% (95% CI, 6.9–16.1%). There was a strong association between placental, cord, maternal and congenital parasitaemia. All babies with congenital malaria had infected mothers and placentas (P<0.01). In conclusion, congenital malaria is still common in Tanzania especially in malaria endemic areas. It is important that blood smear from neonates are taken and examined for malaria parasite soon after birth. Malaria prevention measures such as intermittent preventive treatment, prompt management of all malaria cases and use of insecticide treated bed nets should be emphasized for all pregnant women. Key words: pregnancy, placenta, congenital malaria, neonate, Tanzania Introduction Malaria affects more than 24 million pregnant women and kills more than one million children each year in sub-Saharan Africa while more than 300 million children get sick of malaria annually (WHO, 2000; Steketee et al., 2001). In Tanzania, malaria is still a major public health problem. It is a leading cause of morbidity and mortality accounting for more than 40% of overall outpatient attendances (MOH, 2002). The population groups that are most at risk are children under the age of five years and pregnant women. Pregnant women are vulnerable because of their reduced natural immunity and they are four times more likely to suffer from complications of malaria than non-pregnant women (Jamieson et al., 1993). The devastating consequences of malaria, however, start before the child is born. Children suffer adverse outcomes related to gestational malaria, placental malaria, and congenital malaria. During pregnancy, the acquired anti-malarial immunity of a woman residing in a malaria-endemic area decreases (Alecrim, 2000). The risk of malaria increases threefold during the second and third trimesters and fourfold during the initial two post-partum months (Diagne et al., 2000). This increased risk of malaria is related to an alteration in the balance of Th1 and Th2 immune factors (Moormann et al., 1999). The result of these immune modifications is that, not only do pregnant women get more malaria; they also get sicker when they get malaria. The increased risk of severe malaria has significant adverse consequences on the developing child (Verhoeff et al., 1999). Many pregnant women suffer from severe anaemia, and even death due to acute malaria (Jamieson et al., 2000). Poor foetal growth, low birth weight, pre-term delivery, miscarriage, stillbirth, increased rate of anaemia during infancy and increased risk for malaria during the neonatal period have been associated with gestational malaria (Polack & Divon, 1992 ; LeHesran et al., 1997; Kuyucu et al., 1999; Moormann et al., 1999; Steketee et al., 2001). Congenital malaria has been documented in malaria endemic areas for many years. Studies in Africa have shown that 7–10% or more of newborns have malaria parasites in their placental blood and significant part of the transmission of parasites from the mother to the child occurs well before the time of delivery (Kamwendo et al., 2002; Mwangoka et al., 2008). It is also estimated that, 6% of all infant deaths in malaria-endemic areas are a result of malaria infection that took place during the child’s prenatal life (Fischer, 2003). This study was conducted to determine the prevalence of congenital malaria among neonates born at the Morogoro Regional Hospital in Tanzania. The study also investigated how factors such as malaria status and maternal parity influence some measures of pregnancy outcome such as birth weight, birth length (Kalanda et al., 2005), gestational age and Apgar score (Larkin & Thuma, 1991). Materials and Methods Study area This study was conductedamong term-pregnant women receiving delivery service at Morogoro Regional Hospital, Tanzania. Morogoro Regional Hospital serves as a referral hospital for 14-district level hospitals, 26 health centres and 240 dispensaries. The region has a population of 1,759,809 (877,236 males and 882,571 females), living in 385,260 households with an average of 4.6 people per household (TDHS, 2005). Malaria is one of the ten most common causes of morbidity in the region. Study design, sampling frame and sample size A cross-sectional survey was conducted among pregnant women reporting for delivery services at the Morogoro Regional Hospital between April and June 2009. The sampling frame comprised all term-pregnant women receiving delivery service at the hospital and their newly born babies (0 – 3 days). Systematic random sampling technique was used to obtain the pregnant women. Every second pregnant woman registered at the labour ward for delivery was selected into the sample until the desired number was obtained. The sample size was determined according to WHO (1991a). Using an expected congenital malaria prevalence rate of 15% (Cot et al., 2002; Mwangoka et al., 2008) and degree of desired precision of 0.05, the sample size of 196 (~ 200) pregnant women was obtained. Blood samples One µl of cord blood was taken from the umbilical vein (about 15 cm from its place of attachment to the placenta) after cleaning the cord with 70% alcohol to avoid mixing the cord blood with the maternal blood. The placenta was cleaned immediately after delivery and multiple aspirations made on the maternal half of the placenta as described by Sowunmi et al. (1996). From the aspirates, thin and thick films were made on clean microscope slides. From each mother and baby, 0.5 mL of venous blood was obtained from the dorsum of the hand within 1 hour of delivery using a 23G needle. Duplicates of thin and thick blood films were then prepared from the placenta, the cord and the periphery blood of the mother and the baby (WHO, 1991b). Blood films from mothers, placenta, cords, and babies were stained with Giemsa within 24 hours of collection. Each film was examined by an experienced laboratory technician at a magnification of x100 under oil immersion. Presence of trophozoites or rings on the blood film was taken as a laboratory evidence of malaria. Parasite counts were done using standard methods (WHO, 1991c). Socio-demographic and malaria prevention data A structured, pre-tested questionnaire was administered to the selected sample of pregnant women to solicit information about socio-demographic, maternal birth order, malaria status at first visit to the antenatal clinic, malaria status at delivery, use of bed nets, child birth weight, child length, gestational age at birth, Apgar score and use of anti-malarial drugs for both acute treatment and/or prevention. The data were collected through face-to-face interview with the pregnant women at their delivery wards. Statistical Analysis Data were compiled, coded and analysed using Statistcal Package for Social Science (SPSS) programme version 11.5. Means, variances and frequencies were used to describe the various parameters. Univariate and multivariate analyses were performed to determine the influence of the various factors on the congenital malaria and other birth outcomes. A difference was considered to be significant at p < 0.05. Ethical Clearance Ethical clearance to use human subjects was obtained from the Sokoine University of Agriculture Human Studies Ethics Committee while approval to conduct the study at the hospital was obtained from the Morogoro Regional Health authorities. All women who participated in the study signed an informed consent form to affirm their willingness to participate in the study. Respondents had the liberty to decline participation or withdraw from the study at any stage without the fear of retribution. Women who tested positive for malaria were treated immediately with antimalarial drugs according to national guidelines. Results The majority of the women (81.0%, 95% CI, 75.6 – 86.4%) were young between the age 20–35 years. About 16.0% (95% CI, 10.9 – 21.1%) of the women were teenagers while only a small proportion (3.0%, 95% CI, 0.6–5.4%) of the mothers were above 35 years old. The study revealed further that, 58.0% of the respondents were homemakers, 32.0% were businesswomen/pretty traders and only a small proportion (7.0%, 95% CI, 3.5–10.5%) was employed for wage. About 33.0% (95% CI, 26.5 – 39.5%) of women involved had a parity of 1, while 29.5 (95% CI, 23.2–35.8%), 20.0 (95% CI, 14.5–25.5%) and 13.0% (95% CI, 8.3–17.7%) of the respondents had parity of 2, 3 and 4, respectively. Only 4.5% (95% CI, 1.6–7.4%) of the respondents had parity of 5 or above. The high maternal parity was reflected in the average family sizes whereby most households (63.0%, 95% CI, 56.3–69.7%) had family size ranging from 3 to 4 people. Majority of women were married (72.5%, 95% CI, 66.3–78.7%) and only few women were single (13.0%, 95% CI, 8.0–17.7%), widowed (4.5%, 95% CI, 1.6–7.4%) or divorced/separated (10.0%, 95% CI, 5.8–14.2%). Most of the married respondents (98.0%, 95% CI, 95.7–100.0%) came from households that were headed by males. Majority of the respondents (89.0%, 95% CI, 84.7–93.3%) had attained only primary school education, while only few women had attained secondary education (2.0%, 95% CI, 1.0 – 3.9%) or post-secondary and/or vocational education (0.5%, 95% CI, 0.0 – 3.9%) (Table 1). The majority (86.0%) of the pregnant women (95% CI, 81.2 – 90.8%) reported to own and use insecticide treated net. Records of malarial status of the pregnant women when they first visited the antenatal clinic indicated that, more than 20% (95% CI, 14.5–25.5%) had malaria. Four percent (95% CI, 1.2 – 6.8%) of the women enrolled into the study were not screened for malaria parasites and their status was not known. The most common malaria parasite species identified were Plasmodium falciparum and Plasmodium malariae. Nine out of 10 mothers who tested positive of malaria were infected. All neonates who tested malaria positive were infected with P. falciparum. Data on parasitaemia was available from 184 (92.0%) of the women. Only 11.5% (95% CI, 6.9 – 16.1%) of the blood samples from the maternal periphery blood were positive. Out of the 190 infants delivered (six mothers had twins), only 4.0% (95% CI, 1.2 – 6.8%) tested positive for malaria parasite. The parasite rate of blood samples collected from the maternal placenta was 7.0% (95% CI, 3.3–10.7%). Only 0.5% of the blood sample collected from the maternal cords tested positive for malaria parasites (Table 2). Majority of the babies (95.1%, 95% CI, 92.0–98.2%) were born at term (37- 42 weeks). Out of the 175 children born at term, only six (3.4%, 95% CI, 0.7 – 6.1%) were malaria positive. Nine (4.9%, 95% CI, 1.8–8.0%) of the newborns were pre-term (< 36 weeks) and out of these, 4 babies tested positive for malaria. None of the babies was born post-term (> 43 weeks). Distribution of the average birth weights of the newborns indicated that, 11.8% (95% CI, 7.2–16.4%) of the babies had average weight below the standard weight of 2.5 kg. Majority of the newborns (86.6%, 95% CI, 82.2–91.0%) had normal average birth weights (2.5-4.4 kg). Only few children (1.7%, 95% CI, 0.1–3.5%) were macrosomic, with average birth weights of ≥ 4.5 kg. Out of the 22 low birth weight children, 4 babies (18.2%, 95% CI, 12.7–23.7%) had malaria parasites. Of the 165 babies born with normal average body weight (2.5–4.4 kg), only 6 (3.6%, 95% CI, 1.0 – 6.2%) children were infected with malaria parasites. None of the macrosomic children were infected with malaria parasites (Table 3). Most of the newborn babies (97.4%, 95% CI, 95.1–99.7%) had normal birth lengths (49.4 – 50.9 cm). Of the 5 children with birth lengths below normal, 2 had malaria parasites. Children who had birth lengths below normal were also pre-term (< 36 weeks) babies. Of the children with normal or above normal birth length, 8 (4.3%, 95% CI, 1.4 – 7.2%) tested positive for malaria parasites. Assessment of the physical performance and adaptation to the external environment at 1st and at 5th minute after birth indicated that, most of the babies (98.5%, 95% CI, 96.8 – 100.0%) scored 7–10 in the Apgar scale. Three babies (1.5%, 95% CI, 0.2 – 3.2%) had a fair score of 4 – 6. None of the newborns scored the lowest range of 0–3 in the Apgar scale. Nine children (4.8%, 95% CI, 1.7 – 7.9%) out of the 187 children who scored 7–10 in the Apgar scale were infected with malaria parasites while only 1 out of 3 babies who scored 4–6 in the Apgar scale was infected with malaria parasites (Table 3). Discussion Maternal age is an important determinant of pregnancy outcome. Under-age women (< 19 years) are usually at increased risk of poor pregnancy outcomes such as pre-term, low birth weight babies and high neonatal mortality (Stewart et al., 2007). Malaria in teenage mothers makes the situation even worse, thus increasing the risk of poor pregnancy outcome. Older women (>35 years) are also at increased risk of pregnancy complications that may lead to poor outcomes. According to Stewart et al. (2007), the appropriate age range to conceive without risks for undesirable outcomes is 20–35 years. Prevalence of congenital malaria is uncertain in many parts of tropical Africa including Tanzania. The prevalence rate of congenital malaria observed in this study lower than rates reported elsewhere in Africa (Ezeoke et al., 1985; Larkin & Thuma, 1991; Akindele et al., 1993; Sowanmi et al., 1996; Fischer 1997). In a recent study in a malaria holo-endemic area of north-eastern Tanzania, Mwangoka et al. (2008) reported a prevalence of 19.1%. The low prevalence rate of congenital malaria observed in this study could be attributed to a relatively high coverage of intermittent preventive treatment (IPT) of malaria, and the use of insecticide treated nets. Most of the women in this study had their IPT administered in the 20th week and 35th week of gestation. In addition, more than 86.0% of the pregnant women (95% CI, 81.2 – 90.8%) reported to have bought and using insecticide treated bed nets. There was a strong association between congenital malaria, placental and maternal periphery parasitaemia, with most infected babies having infected mothers and placentas. Larkin & Thuma (1991) reported a similar observation. The significance of this association is that, maternal and placental malaria could result in premature delivery, low birth weight and symptomatic congenital malaria (Lindsay et al., 2000). There was a strong association between placental and cord blood parasitaemia and congenital malaria. Out of 13 women who had malaria parasites in their placenta, eight delivered babies who had malaria parasites at birth. Placental parasitaemia rate of 7.0% is comparable to the rate (9.8%) reported by Mwangoka et al. (2008) from a study in north-eastern Tanzania. Reported prevalence rates of placenta parasitaemia in malaria endemic regions of sub-Saharan Africa are highly variable. Studies in Tanzania and Kenya have reported higher prevalence of placental parasitaemia of 75.5% and 64%, respectively (Menendez et al., 2000; Shulman et al. (2001). Likewise, placental malaria prevalence rates of 9.5%, 18.5%, 19.5% and 37.1% have been reported in Senegal (N’dao et al., 2006), Sierra Leone (Morgan, 1994), Cameroon (Tako et al., 2005) and Gambia (Okoko et al., 2002), respectively. Prevalence of placental malaria also varied greatly from one area to another within the same geographical location. Significant variations in risk and severity of malaria infection have been reported between women in their first pregnancy and women with multiple pregnancies. In this study, out of 10 women who were malaria positive, 6 were primipara, while 2 were para-2, 1 para-3 and 1 para-4. Prevalence of malaria during pregnancy was higher among primipara than among their multipara counterparts. Primipara mothers were therefore more likely to contract malaria than their multipara peers. Shulman et al. (1996) showed that, the risk and severity of malaria infection decreases in proportion to the number of pregnancies, which suggests that, the immune build-up is achieved after several pregnancies and infections. According to McGregor (1984), placenta is immunologically malaria-naïve and it requires a long period of exposure before the maternal immune system can recognize the placenta-sheltered parasites and respond appropriately. Menendez et al. (2000) suggested that, the parasites can temporarily evade the immune system by hiding within the vascular placenta found only in pregnant women. This implies that, while peripheral circulation can be free of parasites, high placental parasitaemia is sometimes observed in infected mothers (Ismail et al., 2000). According to Rasheed et al. (1993), placental synthesis of immunosuppressive factors – estrogens and cortisol act with more vigour locally, thereby allowing the parasites to thrive. This suggests that, the reduction of cortisol and oestrogen levels observed in mothers with high parity reduces their vulnerability to malaria infection. According to Fried et al. (1998), multigravid mothers develop malaria antibodies, which block adhesion of parasites to chondroitin sulphate-A receptor in the placenta in the subsequent pregnancies. A study by Mwangoka et al. (2008) in Muheza district, Tanzania showed that, prevalence of placental parasitaemia decreased significantly as gravidity increased and infants born to primigravid mothers were significantly more likely to be infected with P. falciparum than their peers born to multigravid mothers. In this study, more primigravid mothers had placental and periphery blood parasitaemia compared to their multigravid peers. This observation was consistent with findings of previous studies in malaria endemic regions where among several factors; gravidity independently influenced the occurrence of placental malaria (Okolo & Ibanesebhor, 1992). The cord parasite rate observed in this study was low and comparable to the rate reported from a study in north-eastern Tanzania (Mwangoka et al., 2008). However, higher prevalence rates ranging from have been reported in other studies elsewhere (Lamikanra, 1993; Egwoyenga et al., 1996). Majority of children in this study were born on term (37–40 weeks). An earlier study conducted in Morogoro reported an average gestational age of 36.96 weeks (Nyaruhucha et al., 2006). Babies delivered before 37 weeks are termed “premature” and are often small-for-gestation-age (SGA) and/or low in birth weight. Only 4.9% of the newborns in this study were born before term. Most of the newborns in this study had birth weights ranging between 2.5–4.4 kg. Similar birth weights have been reported in earlier studies in the same region (Kinabo, 1993; Nyaruhucha & Msimbe, 1993; Nyaruhucha et al., 2006. Higher prevalence rates of low birth weights have been reported from studies in Mwanza and Dar es Salaam (Walraven et al., 1997; Kidanto et al., 2006). In light of the above, there was no likelihood that the birth weights of the newborns were affected by the presence of congenital malaria. Results of the Apgar test indicated that, only three children had difficulties to adapt to the new environment and required medical attention. All other children adapted well to the new environment (Hirsch, 2008). The low Apgar score observed in this study is likely to be a reflection of intra-uterine growth retardation (Polack & Divon, 1992). In conclusion, findings of this study indicate that, congenital malaria is a common public health problem in malaria endemic areas of Tanzania. This calls for the need to intensify efforts to protect pregnant women from malaria infections. The importance of effective control measures cannot be over-emphasized because apart from the adverse perinatal outcomes associated with congenital malaria, babies born to mothers with placental malaria are also at a higher risk of contracting severe malaria infections in their first two years of life. Acknowledgements The authors acknowledge with thanks the financial support provided by the Sokoine University of Agriculture, Morogoro. We also extend many thanks to the mothers for generously accepting to participate in this study. Many thanks are also due to the Regional Medical Officer and the Morogoro Regional Hospital Superintendent for granting us permission to conduct the study and for providing some logistical and administrative support. References
Copyright 2010 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th10033t2.jpg] [th10033t3.jpg] [th10033t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}