 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Journal of Health Research, Vol. 12, No. 4, Oct, 2010, pp. 286-289 Short Communication The aetiology, management and clinical outcome of upper gastrointestinal bleeding among patients admitted at the Kilimanjaro Christian Medical Centre in Moshi, Tanzania Mwanahawa R. Suba, Segni M. Ayana, Charles M. Mtabho*, Gibson S. Kibiki Department of Internal
Medicine, Kilimanjaro Christian Medical Centre, Tumaini University, and
Kilimanjaro Clinical Research Institute, P.O. Box 3010 Moshi, Tanzania Received 12
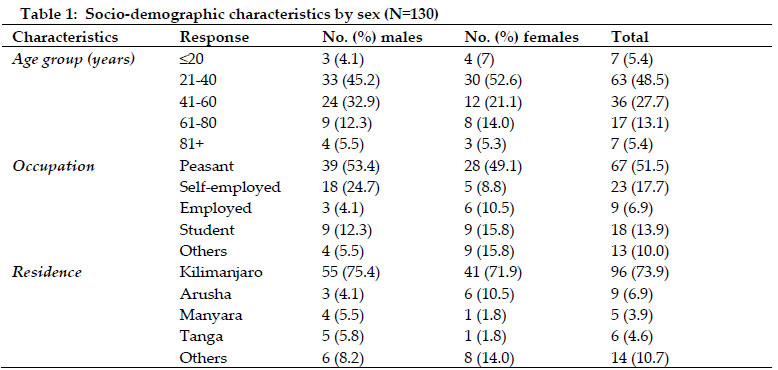
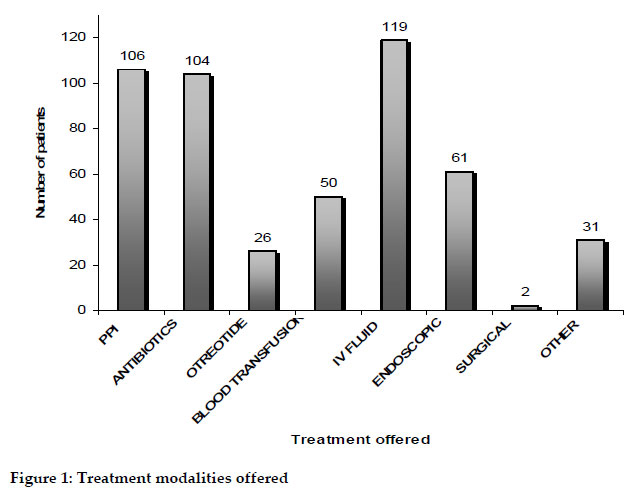
February 2010 Code Number: th10041 Abstract Upper gastro-intestinal (GI) bleeding is a life-threatening emergency that results in high morbidity and mortality and therefore requires admission to hospital for urgent diagnosis and management.The aim of this study was to determine the causes of upper GI bleeding and clinical outcome of patients admitted to medical department with the diagnosis of upper GI bleeding. A retrospective study of records of all upper GI bleeding patients who were admitted to medical department, Kilimanjaro Christian Medical Centre (KCMC) from January 2007 to December 2008 was conducted. A total of 130 patients (13-96 years old) were enrolled in the study, whereby 73 (56.2%) were males. The causes of bleeding, all endoscopically diagnosed included oesophageal varices in 55 (42.3%) cases, followed by duodenal ulcers 20 (15.4%), hemorrhagic/erosive gastritis 10 (7.7%), gastric ulcer 6 (4.6%) and Mallory Weiss tear 2 (1.5%). No cause was identified in the remaining 27 % of cases. Conservative medical therapy alone was carried out in 52.3% of the patients. Endoscopic therapy was used in 61 (46.9%) of patients. Only 2 (1.5%) patients underwent surgical intervention. The overall mortality at discharge was 17%, while 107 (82%) patients were discharged improved. In conclusion, the commonest causes of upper GI bleeding are oesophageal varices and duodenal ulcer. Most cases of upper GI bleeding were successfully treated with pharmacologic and endoscopic treatment. The high mortality may be influenced by delayed presentation to health facilities, and comorbidities. There is a need for strengthening preventive programmes and conducting studies to identify predictors of outcome of upper GI bleeding to develop evidence based management protocols. Keywords: Upper GI bleeding, aetiology, endoscopy, outcome, Tanzania Globally, upper gastro-intestinal (GI) bleeding continues to be a common cause of hospital admission and results in high morbidity and mortality (Cello et al. 1987; Longstreth 1995). Although upper GI bleeding is among the common causes of admission to many hospitals in Africa (Harries & Wirima, 1989; Kibiki et al., 2003; Mustapha et al., 2009), epidemiological surveys from this population are limited. Previous studies in northern Tanzania showed that acute upper GI bleeding is an important cause of hospital admissions and the leading causes are oesophageal varices, oesophagitis, oesophageal ulcers, gastritis, gastric ulcers, duodenitis, duodenal ulcer, and Mallory Weiss syndrome (Kibiki et al., 2003). Predisposing factors for upper GI bleeding include schistosomiasis, congenital hepatic fibrosis, nodular regenerative hyperplasia, heart failures with tricuspid incompetence (which all cause portal hypertension), and peptic ulcer disease (Kumar & Clark, 2002). Endoscopy plays a pivotal role in the diagnosis and management upper GI bleeding. Nevertheless, despite the development of new therapeutic tools such as the proton pump inhibitors, endoscopic interventions and surgical approaches, the overall clinical outcome of the patients has not changed significantly and mortality rate remains around 10% (Vreeburg et al. 1997). There is no local data regarding the causes and clinical outcome of upper gastrointestinal tract bleeding in Tanzania. The aim of this study was therefore to fill this knowledge gap. We retrospectively studied consecutive records of patients who were admitted to the Medical Department for upper GI bleeding and underwent diagnostic endoscopy, from January 2007 to December 2008 at the Kilimanjaro Christian Medical Centre (KCMC). KCMC is a teaching and referral hospital located in the Moshi Municipality in northern Tanzania. It serves over 11 million people in northern Tanzania, but also many patients from central, eastern and western zones of the country. Data on aetiology, management, and clinical outcome was collected from patient files at the Medical Records department. Information on demographic characteristics, endoscopic findings, medical and/or surgical management and condition at discharge of all patients were recorded in standardized format. Permission to conduct the study was obtained from KCMC Ethical Committee. A computer software package SPSS version 14 was used for data management and analysis. Results were summarized in frequency distribution tables, charts and figures. A total of 130 patients were enrolled in the study. Seventy three (56.2%) were males (male to female ratio 1.2: 1). Their ages ranged from 13 to 96 years with a median age of 39 years (interquartile range: 28-53 years). Socio-demographic characteristics are summarised in Table 1. Of the 130 patients with upper GI bleeding, in 55 it was due to oesophageal varices, 40 non-variceal causes, and in 35 patients the cause was not identified. The endoscopical grades of patients who had variceal type of upper GI bleeding were grade I, 2 (3.6%) patients, grade II 13 (23%), grade III 14 (25.5%), and grade IV 26 (47%). The frequency of non- variceal causes of upper GI bleeding were duodenal ulcer 20 (50%), haemorrhagic/erosive gastritis 10 (25%), gastric ulcer 6(15%), Mallory Weiss syndrome 2 (5%), and duodenitis 2 (5%). Sixty two patients (47.7%) were offered conservative medical treatment only, including intravenous fluid replacement with normal saline and Ringer’s lactate, intravenous proton pump inhibitors, IV octreotide, antibiotics and blood transfusion as appropriate (Figure 1). Endoscopic treatment was performed in 61 (46.9%) of patients. This included endoscopic injection of sclerosant to oesophageal varices with polidocanol and peri-lesional injection of epinephrine (1:10,000) to bleeding peptic ulcers. Only 2 (1.5%) patients were subjected to surgical intervention. Majority of patients (82%) improved clinically after treatment whereas 22 (17%) patients died, and only one (1%) had his condition worse at discharge. The present study was carried out at teaching hospital to obtain basic information on the socio-demographic, causes, management and clinical outcome of patients with upper GI bleeding with intent to shine light on this major cause of morbidity and mortality at our centre. Comparisons of the present retrospective study with previous studies from other cities or countries may be confounded by variations in methodology, definitions and entry criteria used as well as by the heterogeneity of the different populations analyzed. In this study, there was a slight male preponderance and this is consistent with findings of Rockall et al. (1995) and Yavorski et al. (1995). A previous study at our centre by Neema J. Rajabu (unpubl) on oesophageal varices, which is the major cause of bleeding in the present study, also showed male predominance. This might be explained by the higher prevalence of underlying illnesses among males, such as liver disease; and higher tendency of alcohol consumption among males. Majority of the study population comprised of peasants. Peasants work in environment favourable for contracting diseases like schistosomiasis which lead to portal hypertension. Similar findings were obtained in a study by Elliott (1996) in which it was found that types of activities and local production patterns determined the exposure of individuals to schistosome-infested water sources. A bleeding site could be detected in about three-fourth of the patients in the present study. This result is similar to that reported in other studies (Rockall et al. 1995; Vreeburg et al. 1997; Zaltman et al. 2002). The time interval between the bleeding episode and the endoscopic procedure are known to influence the accuracy and the likelihood of finding a cause endoscopically (Zaltman et al. 2002). In our study, the most common bleeding lesion identified at upper endoscopy was oesophageal varices. This is consistent with findings of other studies (Harries & Wirima 1989; Kibiki et al. 2003) but different from studies in UK (Rockall et al. 1995), Netherlands (Vreeburg et al. 1997) and Brazil (Zaltman et al. 2002) where bleeding duodenal ulcer was the commonest endoscopic finding. This difference could be explained by the known high prevalence of schistosomiasis in our set up which is a known risk factor for oesophageal varices (Kitange et al., 1993). In the present study, duodenal ulcer was the leading cause of non-variceal upper GI bleeding. There is definite role for Helicobacter pylori infection in the etiopathogenesis of duodenal ulcer (Chan et al. 2002). This finding could probably be due to the high prevalence of H. pylori infection in the population (Aoki et al. 2004). However, we could not determine the prevalence of the infection in this retrospective study, because tests for H. pylori status were not routinely made in patients with acute upper GI bleeding during the period. The overall mortality rate in the present study (17%) is consistent with studies by Zaltman et al. (2002) in Brazil and by Chojkier et al. (1986) in the USA but higher than study by (Yavorski et al. 1995) in the USA. The high mortality could be due to delayed presentation to health facility and a pre-selection of high-risk patients with significant underlying medical conditions, to an academic and referral medical centre; but could also be partly compounded by comorbidities. Acute upper GI bleeding is a life threatening emergency. However, the accessibility of the patients to medical centres with experienced medical staff and adequate equipment is still limited in Tanzania. Moreover, it is possible that many patients are admitted late in the course of the bleeding episode, while others may never reach the hospital. As it occurs in other retrospective studies, loss of data is frequent and sometimes blunts the retrieval of fundamental information. Failure to document information or loss of information in the emergency room and medical wards, as well as loss of endoscopy records resulted in lack of recorded information in several areas and serves as an advice to the need for improving the quality and consistency of recording in different units. In conclusion, oesophageal varices is the major cause of upper GI bleeding and that upper GI bleeding is associated with high mortality. In this retrospective study we have confirmed that endoscopy contributes to identifying the bleeding site in most patients and successful treatment. There is a need for strengthening preventive programmes and conducting studies to identify predictors of outcome of upper GI bleeding to develop evidence based management protocols for subsequent reduction of the morbidity and mortality associated with the illness. References
Copyright 2010 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th10041t1.jpg] [th10041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}