 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Journal of Health Research, Vol. 13, No. 1, January, 2011, pp. 79-86 A retrospective study of Human African Trypanosomiasis in three Malawian districts John E. Chisi 1, Adamson S. Muula2*, Bagrey Ngwira 2 and Stone Kabuluzi 3 1Department
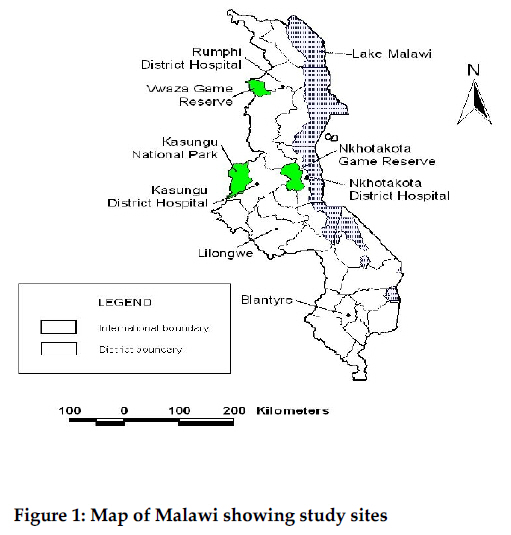
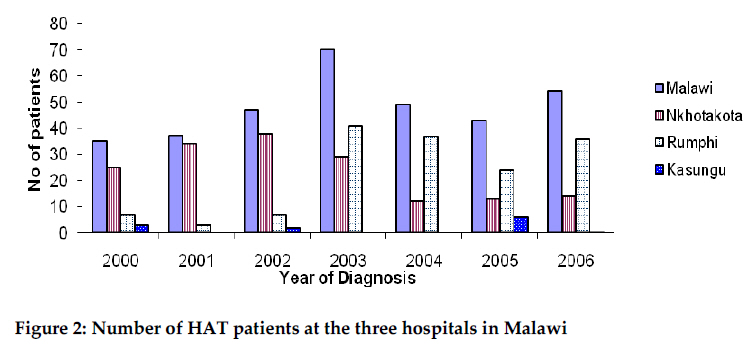
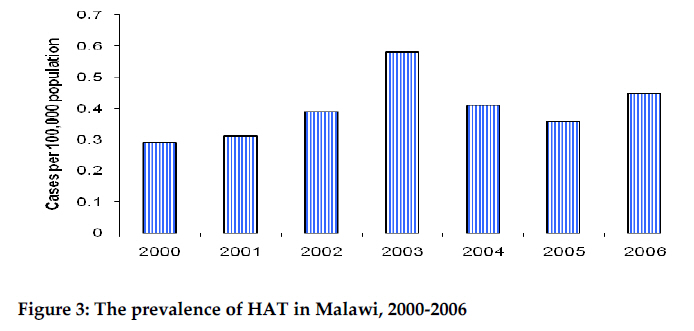
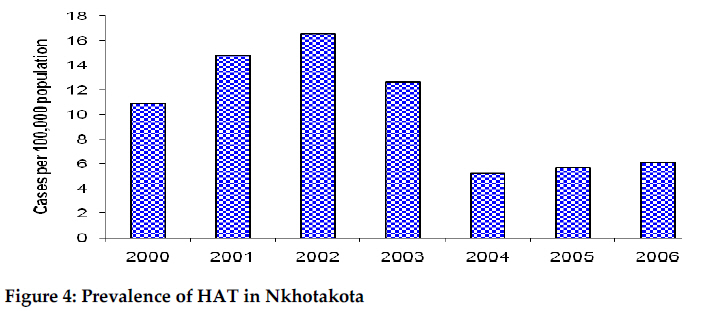
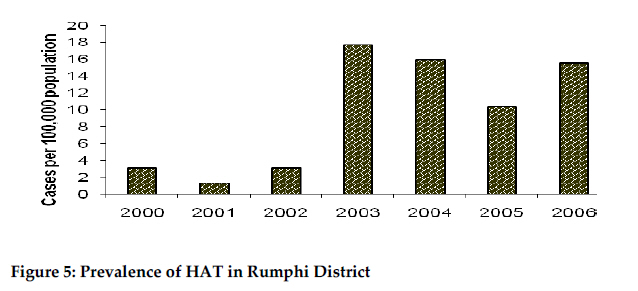
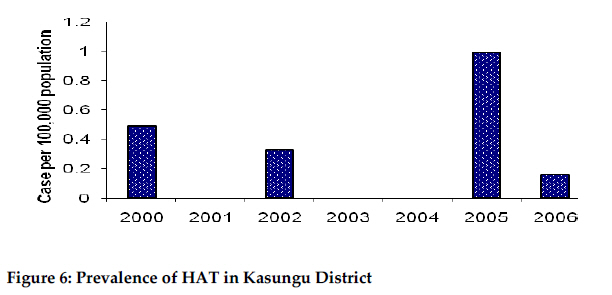
of Haematology, College of Medicine, University of Malawi, Blantyre, Malawi Code Number: th11010 Abstract Human African Trypanosomiasis (HAT) is a neglected tropical disease (NTD). Surveillance in many of the endemic areas is often inadequate. Up to date information on the HAT situation in Malawi, where the disease is endemic in some districts, provides opportunity to raise the profile of the disease and interest in prevention and control. A retrospective study was conducted in three Malawian districts: Nkhotakota, Rumphi and Kasungu to describe the prevalence of HAT. Hospital laboratory registers from January 2000 to December 2006 were used. The calculated annual district prevalence of Trypanosomiasis ranged from 0.29 cases per 100,000 population in 2000, to 0.58 cases per 100,000 population in 2003. Nkhotakota District had the highest case detection rate of trypanosomiasis of 16.56 cases per 100,000 in 2002 and the lowest rate in 2004 of 5.23 cases per 100,000. From 2004 onwards a decline in cases detected was observed. In Rumphi district the highest number of cases (17.67 cases per 100,000 population) was identified in 2003 and the lowest rate of 1.29 cases per 100,000 in 2001. The rate (17.67 cases per 100,000) found in 2003 represented a 5-fold increase of 2002 (3.02 cases per 100,000). In Kasungu the detection rate ranged from 0 per 100,000 in 2001, 2003 and 2004 to 0.99 cases per 100,000 in 2005. The number of cases in this district has remained low including in 2006, when a detection rate of 0.16 cases per 100,000 was observed. HAT is endemic in selected districts of Malawi. There is need to explore the feasibility of active disease surveillance and the establishment of permanent preventive and control measures. Keywords: Human African trypanosomiasis, Tsetse fly, Glossina, Malawi Introduction Human African Trypanosomiasis (HAT) is a vector-borne disease currently classified among global neglected tropical diseases (NTDs). Individual clinical treatment and public interest in the disease is limited compared to other infectious diseases or vector-borne diseases such as malaria, tuberculosis and HIV. Several districts in Malawi are known to be endemic to HAT. However, the prevalence of the disease in the affected districts is largely unknown. Recently there has been sporadic surveillance activities conducted in several districts in the country dependent on availability of funds (Chisi et al., 2003). Little attention has been paid to this disease possibly as it is mainly restricted to rural-remote (hidden) areas surrounding ‘natural’ game parks and reserves. Patients with HAT are usually stigmatized and often considered deserving of infection for entering game parks without official government permission. This may act as barrier for them to report to health facilities to seek care. HAT is caused by a subspecies of extracellular hemiflagillate of Trypanosoma brucei found in East and West Africa. The East African subspecies, Trypanosoma brucei rhodesiense (T. b. rhodesiense) generally causes an acute infection, while the West Africa subspecies i.e., Trypanosoma brucei gambiense (T. b. gambiense), causes a more chronic disease lasting several years if no effective treatment is given. Recent studies have shown that T. b. rhodesiense disease found in Malawi and possibly Zambia tends to last for a longer period than that found in Uganda (Maclean et al., 2004). Trypanosomiasis is transmitted by Tsetse flies (Glossina spp). The reservoir hosts for these parasites are generally wild animals; domestic animals have also been implicated (van den Bossche, 2001). Tsetse flies were first reported as vectors for HAT in Malawi in 1903 in the then British colony of Nyasaland (Austen, 1903). The most common species of tsetse flies that transmit trypanosomes in Malawi is Glossina morsitans morsitans, which are mostly found in and around Kasungu National Park, and game reserve of Vwaza (Mzimba and Rumphi) and Nkhotakota districts (Mitchell & Steele, 1956; Davison, 1990). More recent data are not available. The HAT patient presents with similar symptoms as those found in patients suffering from malaria and in some cases the disease might present with signs and symptoms of immune-suppression (Bell, 1995). Since the symptoms are non specific, it is generally difficult to make a diagnosis in resource poor settings with limited laboratory diagnostic facilities as is usually the case in rural Malawi. This study was conducted to estimate the prevalence of HAT in 3 districts that border game reserves known to be infested with G. morsitans morsitans. Materials and Methods A retrospective study was carried out in three Malawian districts of Rumphi, Kasungu and Nkhotakota using hospital laboratory registers. For each patient who was identified to be infected in the hospital laboratory register, the case notes were retrieved. The data were then extracted from case files. As all acute cases of HAT in the districts are usually admitted to the respective district hospitals where treatment is given, the data were deemed to be representative of the disease pattern in the districts concerned with regard to all reported cases. Rumphi is a district in northern Malawi bordering Karonga to the North, Nkhatabay to the East, Zambia and Chitipa to the West and Mzimba district to the South. It had an estimated population of 232,011 people (National Statistical Office, 2004). Vwaza game reserve is located within the boundary of Mzimba (Malawi) and Zambia. Here Glossina morsitans morsitans and Glossina pallidipes are prevalent (Mitchell & Steele, 1956; Davison, 1990). Kasungu is a district in the central region of Malawi which borders Nkhotakota to the East, Zambia to the West, Mzimba to the North and Dowa to the South. It had a population of 608,917 people (National Statistical Office, 2004). Kasungu national park is located on its border with Zambia. This park is also highly infested with G. morsitans morsitans. Nkhotakota has Nkhatabay in the North East, Mzimba to the North West, Kasungu to the West, Ntchisi to the South West and Salima to the South East. It had a population of 229,460 people (National Statistical Office, 2004). Nkhotakota district has Nkhotakota game reserve which borders Kasungu and Ntchisi districts (Figure 1). The game reserve is similar to the other two parks infested with G. morsitans morsitans. Records reviewed were compiled from the period January 2000 to December 2006. All cases included were those of HAT that had been diagnosed and treated at hospitals. The diagnosis of HAT was made on the basis of finding trypanosomes on a thick blood film using Giemsa or field stain techniques. All investigations were carried out by trained laboratory technicians who served in the district hospital laboratories. The laboratory findings were cross checked with the case files that were kept at the registry office. Only cases that had smear positive results for trypanosomes were included in this study. The data were then compared to that of the National Trypanosomiasis Control Programme that was kept at the Central Health Sciences Unit (CHSU). Results In the studied period, 335 cases of HAT were recorded in the CHSU register. Nkhotakota recorded 165 cases, Rumphi 155 cases and Kasungu 12 cases; the district of origin of three cases from the CHSU register could not be identified. The absolute numbers of HAT cases were detected and recorded for the country data from the CHSU register. Overall the highest numbers were identified in 2003 (Figure 2). In this year, there were 70 cases of HAT detected and recorded in the whole country. Of these, 29 were identified from Nkhotakota district hospital records while 41 were identified from Rumphi district hospital records. In contrast the year 2000 had the least number of cases detected, with 25 cases identified in Nkhotakota district, seven in Rumphi district and three in Kasungu district. Rumphi district hospital had registered the highest number of cases in one year at 41. Nkhotakota never reported less than 10 cases per year during the entire study period while Rumphi had less than 10 cases per year detected between 2000 and 2002. Kasungu case detection was below 10 cases per year during the whole study period. The case detection rate of HAT ranged from 0.29 (population denominator of 12 million people) cases per 100,000 in 2000 to 0.58 cases per 100,000 in 2003. The number of cases detected increased from 2000 to 2003, since then there has been a steady decline in cases detected annually. However, the case detection rate has never been below 0.3 cases per 100,000 (Figure 3). When individual districts were analyzed, Nkhotakota had its highest case detection rate in 2002 when the records showed a rate of 16.56 cases per 100,000. The lowest rate was found in 2004 when only 5.23 cases per 100,000 were noted. From 2000 to 2003 (inclusive), the district rates of HAT were above 10 cases per 100,000 per year. However from 2004 to 2006 a decline of detected cases was observed as the prevalence never exceeded 6.5 cases per 100,000 per year (Figure 4). Rumphi district records revealed its highest case detection rate of 17.67 cases per 100,000 in 2003 and the lowest rate of 1.29 cases per 100,000 in 2001. Of note the detection rate was below 5 cases per 100,000 per year from 2000 to 2002 (inclusive). There was however an increase in the number of cases of HAT between 2003 and 2006. During this period a 5-fold increase in the case detection rate from 3.02 cases per 100,000 in 2002 to 17.67 cases per 100,000 in 2003 was observed. In addition the rate remained above 10 cases per 100,000 per year (Figure 5) after the initial peak in 2003 to the end of the study period. No decline was observed in the prevalence of HAT in the district from 2003 to 2006. Kasungu district had the lowest number of cases of HAT during the study period when compared to both Nkhotakota and Rumphi districts. The case detection rate ranged from 0 per 100,000 in 2001, 2003 and 2004 to 0.99 cases per 100,000 in 2005. The rate has remained low in the district during the entire study period. In 2006 a detection rate of only 0.16 cases per 100,000 was found. In absolute terms the numbers have never exceeded 6 cases of HAT per year in the district over the past 5 years (Figure 6). Out of the 14 people that were identified with HAT in Nkhotakota in 2006, five died (case fatality 36%), three of them died in the ward and two died at home. Of the discharged patients, one died three months after discharge from the hospital and the other six month later. In 2006, Rumphi identified 36 cases of HAT, of these three people died while in hospital (case fatality 8%). No records were available for the patients that were discharged. Kasungu had identified one case in 2006 with no outcome data. In all cases, treatment was Suramin in the first stage and Melarsoprol B with Suramin and Prednisolone in the second stage. Discussion Several districts in Malawi are endemic of HAT. However, data on HAT epidemiology in Malawi are largely absent. The present study shows that HAT is endemic in the three Malawian districts studied. Sadly, morbidity and mortality rates of this disease remain largely unknown as there is little active surveillance being carried out. Most of the HAT patients are treated for malaria or immunosuppression as the index of suspicion of HAT among medical personnel is generally low. Data from years prior to this study kept at CHSU show that cases of HAT have also been reported in Ntchisi district next to Nkhotakota game reserve, Chikhwawa district in the Southern region and Mzimba district which borders Vwaza game reserve (Chisi et al., 2003). However, since 2000 to 2006, it is only the three study areas which have reported cases of HAT. The data presented here shows that Malawi had the highest prevalence of HAT in 2003. Currently trends in prevalence are showing a reduction in cases in Nkhotakota but an increase in Rumphi. The reasons for this trend are unclear. From 2001 to 2003, Nkhotakota district hospital had a Wellcome Trust funded project studying anaemia caused by HAT (Chisi et al., 2004). This project helped train Health Surveillance Assistants in health education pertaining to HAT. As a result an increased number of cases were detected between 2000 and 2003. Once funds were exhausted, there was no further concerted public health awareness activities related to this disease. Moreover, staff that had been trained for HAT activities, both in the laboratory and clinical setting, left the district hospital for other jobs. The data show the positive impact that this project had on case detection. It is possible however that the reduction in number of cases could be due to a drop in the number of cases in the community, or as previously postulated due to a lack of ability to actively detect new cases of HAT by the regular district health services. The second scenario is probably the most likely one as currently Nkhotakota district hospital does not have adequate human resource capacity to detect and manage cases of HAT. Rumphi hospital is showing an opposite trend to the one seen in Nkhotakota. Fewer cases were detected before 2002 as shown by the low case detection rates. However, a steady increase in the rate of HAT can be observed from 2003 on wards. Recently, there has been an active health education programme on trypanosomiasis in this district and Health Surveillance Assistants have been supplied with motor bikes to help delineate the foci of the disease. Malawi has also recently joined the East African Network for Trypanosomosis (EANETT). This network has provided resources for training in case detection in all the three study districts. The increased knowledge about HAT may have further contributed to the increased numbers of cases recorded. At Kasungu district hospital very few cases were reported during the study period despite a larger case load being detected in the past (Chisi et al., 2003). The case that was detected in 2006 was detected during EANETT funded training. The patient was in the ward, being treated for another condition. It is therefore likely that most cases which have presented at Kasungu district hospital in the past have not been diagnosed. This observation is strengthened by the fact that a British soldier was diagnosed with HAT outside Malawi after training at Kasungu National Park (Croft et al., 2006; 2007). In addition, there have not been any interventions to stop the transmission cycle of HAT in areas in and around Kasungu national park yet the cases detected have been low indicating that the true extent of HAT cases in the community remains unknown. Surprisingly, in 2005 the prevalence of HAT was higher compared to other years. The reason for this increase in detection activity is currently unknown to us. The absolute numbers recorded in the district were generally low during the study period. This study has a number of limitations. The present study reported on data from three selected districts in Malawi. In our estimation of prevalence, we used total district population when probably the population of “at risk” communities would have provided a better denominator. However, while the district human population estimates can be readily obtained from the National Statistical Office, realistic “at risk” population will need to be calculated specifically for the purpose. We were not able to do that. A second limitation concerns the fact that comprehensive socio-demographic data were not accessed, to derive a more in-depth picture of the epidemiology of the disease. Future studies should be designed with prospective data collection to collected relevant socio-demographic data. Another limitation in the present study is the lack of comprehensive laboratory techniques used in the study districts i.e. only Giemsa and/or Field’s stain in thick smear which may end up missing a number of cases. Other simple techniques such as wet smear and haematocrit centrifugation techniques could have improved diagnosis and should be introduced. Finally, the fact that laboratory diagnosis of cases occurs at the district hospital may lead to missing of cases at local community health centres. In conclusion, the present study has shown that HAT control and detection in Malawi is very much under developed. It is obvious that Malawi has a HAT problem and if resources were available the detection, treatment and follow up of treated cases could reduce the burden of the disease as shown partly by the Nkhotakota district hospital data. More financial and human resources are needed in order to conduct surveillance, health education and treatment of the disease. Above all, the extent of HAT in Malawi remains largely unknown unless detailed studies can be carried out. There is need to consolidate resources so that further epidemiological studies can be done, and a more accurate picture of the disease established. Acknowledgements To Kathrin Broetz-Chisi for editing the script, Eastern African Network for Trypanosomiasis for funding the research and to District Health Officers (DHOs) of the 3 districts hospital for encouraging us to conduct this research and staff of the laboratories for data collection and record keeping. We are also grateful to Government of Malawi through Central Health Sciences Unit (CHSU) for providing logistical support. References
Copyright 2011 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th11010f6.jpg] [th11010f4.jpg] [th11010f3.jpg] [th11010f2.jpg] [th11010f5.jpg] [th11010f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}