 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
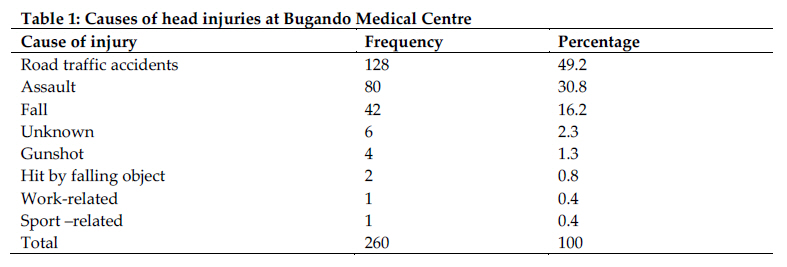
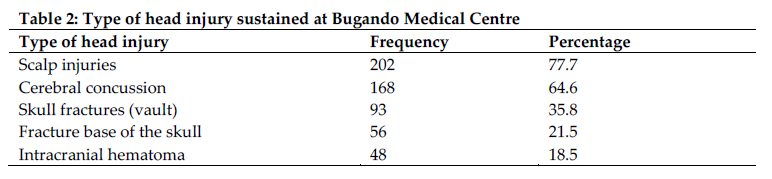
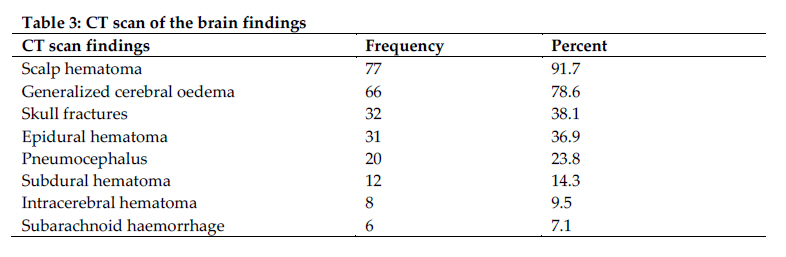
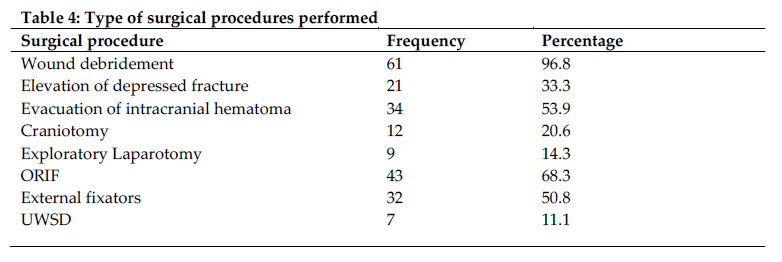
Tanzania Journal of Health Research, Vol. 13, No. 1, January, 2011, pp. 93-102 Aetiological spectrum, injury characteristics and treatment outcome of head injury patients at Bugando Medical Centre in north-western Tanzania Phillipo L. Chalya*, Emmanuel S. Kanumba, Joseph B. Mabula, Godfrey Giiti and Japhet M. Gilyoma Department of Surgery, Weill-Bugando University College of Health Sciences, Mwanza, Tanzania Code Number: th11012 Abstract Head injury is considered as a major health problem that is a frequent cause of death and disability and makes considerable demands on health services.A cross-sectional study was conducted to determine the etiological spectrum, injury characteristics and treatment outcome of head injury patients at Bugando Medical Centre (BMC) in North-western Tanzania. Data were collected using a pre-tested, coded questionnaire and analyzed using SPSS programme. A total of 260 head injury patients (mean age=26.84 years) were studied. Males outnumbered females by a ratio of 1.5:1. Road traffic accidents (RTAs) were the most common cause of injury accounting for 49.2% of patients. Scalp injuries, cerebral concussion and skull fractures were the most common type of head injuries. Fifty-six (21.5%) patients had associated injuries of which musculoskeletal region (36.1%) was commonly affected. Most of patients (66.1%) sustained mild head injury. The majority of patients (75.8%) were treated conservatively and only 24.2% of patients needed surgical interventions. Most of patients (85.4%) had good recovery. The mean hospital stay (LOS) was 24.56 days and the mortality rate was 11.2%. Patients who had RTAs, penetrating head injuries, associated long bone fractures and those who were treated surgically were found to have significantly longer LOS (P< 0.001). Mortality was found to be significantly associated with extreme of age, presence of pre-morbid illness and associated injuries, admission Glasgow Coma Score < 9, systolic blood pressure < 90mmHg, injury severity core ≥16, longer duration of loss of consciousness, the need for intensive care unit admission and finding of space occupying lesion on computed tomography scan (P < 0.001). Head injuries resulting from RTAs remain a major public health problem in this part of Tanzania. Urgent preventive measures targeting at reducing the occurrence of RTAs is necessary to reduce the incidence of head injuries in this region. Key words: aetiology, spectrum, head injury, treatment outcome, Tanzania Introduction Head injury is recognized as a major public health problem worldwide and it is associated with high morbidity and mortality both in developed and developing countries (Thurman & Guerrero, 1999; Guerrero et al, 2000; Kay & Teasdale, 2001; Emejulu & Malomo, 2008; Agrawal et al, 2009). In developing countries including Tanzania, injuries in general and head injury in particular are increasing due to increase in urbanization, motorization, civil violence, wars and criminal activities (Mbembati et al, 2009). In Bugando Medical Centre in Mwanza, Tanzania, head injuries is the single most common cause of trauma admissions and contribute significantly to high mortality and long-term disabilities (BMC Medical record database, 2008-2009). The causes and pattern of head injuries have been reported in literature to vary from one part of the world to anotherpartly because of variations in infrastructure, civil violence, wars and crime (Laleef & Abedayo, 2007). Road traffic accidents (RTA) are the commonest cause of blunt head injuries in civilian practice accounting for up to 70% in some series and are especially common in teenagers and young adults (Foulkes et al 1991; Marik et al, 2002). Falls are responsible for the next largest group of injuries and are more common at the extremes of age. Alcohol has been shown to be a contributing factor in approximately 40% of all severe head injuries (Marik et al, 2002; Yattoo & Tabish, 2008). Head injuries are often associated with other extra-cranial injuries (Laleef & Abedayo, 2007, Foulkes et al 1991). The management of patients with head injury is complex and requires a coordinated, comprehensive and multidisciplinary approach. The goal of management of head injuries is prevention of secondary brain injury by avoiding hypotension and cerebral hypoxia. Early recognition and treatment of surgically correctable intracranial lesion along with prompt treatment of associated extra-cranial injuries is essential for optimal patient outcome (Marik et al, 2002; Yattoo & Tabish, 2008). However, lack of pre-hospital care, ineffective ambulance system and lack of trauma centres coupled with poor infrastructure and increased criminal activities in our setting are major challenges in provision of optimal care to these patients. This calls for urgent planning of preventive strategies to address these challenges. Majority of head injuries are preventable. A clearer understanding of the causes, injury patterns and outcome of these patients is essential for establishment of preventive strategies as well as treatment protocols. Such data is lacking in our environment as there is no local study which has been done. The objective of this study was to determine the etiological spectrum, injury patterns and outcome of head injuries in our setting. The study results will provide basis for planning of preventive strategies and establishment of treatment protocols. Materials and Methods Study design and subjects This was a cross sectional study, carried out at the Accident and Emergency of Bugando Medical Centre over a 2- year period between April 2008 and March 2010. Bugando Medical Centre is a consultant, teaching and referral hospital with a bed capacity of 1000. A description of the hospital and its Accident and Emergency (A&E) department has been described previously by Chalya et al. (2010). All head injury patients who presented to the A & E department during the study period were, following informed consent, consecutively recruited into the study. Patients who died before initial assessment and those without next of kin to consent were excluded from the study. Head injury was defined as both blunt and penetrating injuries affecting the cranium and its contents. Recruitment of patient to participate in the study was done at the A&E department after primary and secondary surveys done by the admitting surgical team. Patients were screened for inclusion criteria and those who met the inclusion criteria were requested to consent before being enrolled into the study. All study patients were first resuscitated in the A&E department according to Advanced Trauma Life Support. From the A & E department patients were taken into the surgical wards or the intensive care unit (ICU) from where necessary investigations were completed and further treatment was instituted. A complete history was taken and a neurological assessment was performed on each patient. The severity of head injury was assessed using Glasgow Coma scale (GCS) taken on admission and patients were classified as GCS of 13-15, 9-12 and 3-8 for mild, moderate and severe head injuries respectively. In addition to GCS, the severity of polytraumatised patients was assessed using Injury Severity Score (ISS). An initial systolic blood pressure (SBP) on each patient was also recorded on admission. Pre-operative skull X-rays in two views (i.e. lateral and antero-posterior) were taken in all patients and others underwent computed tomography (CT) scan according to the type and severity of injury. Associated injuries were investigated accordingly. The diagnosis of head injury was made by clinical history, physical examination and abnormal skull radiographs and CT scan. Depending on the type of injury, the patients were treated either conservatively (i.e. close observation, antibiotics, anti-oedema measures, and anti-epileptics etc) or by surgery (i.e. surgical debridement of scalp lacerations, craniotomy, evacuation of hematoma and treatment of associated extra-cranial injuries). Patents were followed up for three months after the injury. The length of hospital stay and mortality as measures of outcome were recorded on discharge or death. The outcome of patients at 3 months after injury was assessed according to the Glasgow outcome scale (GOS) and categorized as: (1) death; (2) persistent vegetative state; (3) severe disability (conscious but disabled); (4) moderate disability (disabled but independent) and (5) good recovery (Teasdale & Jennett, 1974). A score of 4 to 5 was considered a favourable outcome (moderate disability or less) and a score of 1 to 3 was considered unfavourable (severe disability or death). Data collection Data was collected using a pre-tested coded questionnaire. Data administered in the questionnaire included details of demographic profile, causes of injury, injury characteristics, injury severity using Glasgow Coma scale (GCS) and injury severity score (ISS), treatment offered, complications, length of hospital stay (LOS), mortality and outcome of treatment at 3 months using Glasgow outcome scale (GOS). Data analysis Data collected was entered into a computer and analyzed using SPSS software version 11.5 with help of a medical statistician. Data was summarized in form of proportions and frequent tables for categorical variables. Continuous variables were summarized using means, median, mode and standard deviation. χ2-test was used to test for significance of associations between the predictor and outcome variables in the categorical variables. Student t-test was used to test for significance of associations between the predictor and outcome variables in the continuous variables. Multivariate logistic regression analysis was used to determine predictor variables that are associated with outcome. Significance was defined as a p-value of less than 0.05. Ethical consideration Ethical approval to conduct the study was obtained from the WBUCHS/BMC joint institutional ethic review committee before the commencement of the study. Informed consent was sought from each patient before recruitment into the study. Results A total of 12140 trauma patients were admitted during the study period of whom 260 (21.4%) had head injuries. There were 158 (60.8%) males and 102 (39.2%) females with males out-numbering females by a ratio of 1.5:1. Their ages ranged from 1 to 82 years with a mean of 26.84 years. Twenty-three (8.8%) patients reported to have pre-morbid illness. These included diabetes mellitus in 7 (30.4%), hypertension in 6 (26.1%), renal disease in 4 (17.4%) and pulmonary tuberculosis 3 (13.0%) and congenital heart disease in 3 (13.0%) patients. The majority of patients (206; 79.2%) sustained blunt head injuries and the remaining 54 (20.8%) had penetrating head injuries. The blunt to penetrating head injuries ratio was 3.8:1. Road traffic accidents (RTAs) were the most common cause of injury accounting for 128 (49.2%) patients (Table 1). Sixty-seven (52.3%) of RTAs were related to motorcycle injuries affecting motorcyclists (32, 47.8%), passengers (18; 26.9%) and pedestrian (7, 10.4%). Helmet use was recorded in only 13 (19.4%) of patients who sustained motorcycle injuries. Penetrating head injuries were mainly due to scalp injuries by sharp weapons. Most of injuries (152, 58.5%) occurred during the day. The vast majority of patients (167, 64.2%) reported to the A & E department within 24 hours after injury. None of the patients received any pre-hospital care and majority of them (203, 78.1%) were brought in by relatives, friends or Good Samaritan, 52 (20.0%) by police and only 5 (1.9%) patients were brought in by ambulance. Fifty-six (21.5%) patients had associated injuries of which musculoskeletal region (39, 36.1%) was commonly affected (Figure 1). A total of 108 (41.5%) patients presented with history of loss of consciousness (LOC). The duration of consciousness was < 30 minutes in 20 (18.5%) patients who had mild head injuries, 30 minutes to 24 hours in 53 (49.1%) patients who had moderate head injuries and > 24 hours in 35 (32.4%) those who had severe head injuries. The mortality rates in patients with duration of LOC < 30 minutes, 30 minutes to 24 hours and > 24 hours were 24.1% (7 deaths), 26.6% (8 deaths) and 48.3% (14 deaths) respectively. These differences were also statistically significant (p-value < 0.001). Three (33.3%) patients had neurological deficits. Bleeding from the ears and nose was observed in 31 (11.9%) of patients. The Glasgow coma scale indicated that most of the patients (172, 66.1%) sustained mild head injury, 53 (20.4%) patients sustained moderate head injury and 35 (13.5%) patients had severe head injury. The mortality rates in patients with mild, moderate and severe head injuries were 13.8% (4 deaths), 24.1% (7 deaths) and 62.1% (18 deaths) respectively. These differences were statistically significant (P< 0.001). Injury severity score (ISS) was calculated in 56 patients who had multiple injuries. The overall ISS ranged from 1– 45 (mean 6.8). The majority of patients sustained mild to moderate injuries (ISS < 16) in 48 (85.7%). Severe injuries (ISS ≥16) occurred only in 8 (14.3%) patients. Patients with ISS ≥ 16 had significant high mortality rate (79.3%) compared with patients who had ISS < 16 (20.7%) (P < 0.001). The majority of patients (212; 81.5%) had systolic blood pressure (SBP) > 90 mmHg on admission and the remaining 48 (18.5%) patients had SBP of 90mmHg and below. Mortality rates in patients with SBP < 90mmHg and those with SBP >90mmhg were 72.4 %( 21 deaths) and 27.6% (8 deaths) respectively. These differences were significant (P < 0.001). Skull X-ray was done in all patients and revealed normal findings in 151 (58.1%) patients. Abnormal findings were detected in 109 (41.9%) patients and these included skull (vault) and maxillofacial fractures in 93 (85.3%) and 16 (14.7%) respectively. Skull (vault) fractures (Table 2) included linear fractures in 51 (54.8%), depressed and comminuted fractures in 26 (27.9%) and 16 (17.2%) respectively. Maxillofacial fractures included mandibular and maxillary fractures in 5(31.3%) and 11(68.7%) respectively. CT scan of the brain and skull was requested in 124 (47.7%) patients, but it was only performed in 84 (32.3%) due to financial problems and other logistics. CT scan revealed single lesion in 30 (35.7%) patients, two lesions in 18 (21.4%), multiple lesions in 14 (16.7%) patients and it was normal in 22 (26.2%) patients (Table 3). The majority of patients (214, 82.3%) were admitted in general surgical wards and the remaining forty-six (17.7%) patients were admitted in the intensive care unit (ICU) where 36 (78.3%) of them were subjected to ventilatory support. The majority of our patients (197; 75.8%) were treated conservatively and 63 (24.2%) patients needed surgical intervention (Table 4). The overall length of hospital stay (LOS) ranged from 1 to 130 days (mean = 24.56 days). The LOS was significantly longer in patients with associated long bone fractures. The LOS for non-survivors ranged from 1 to 18 days (mean= 7.84 days). The LOS in the ICU ranged from 1 to 34 days (mean= 7.34 days). Patients who had RTAs, penetrating head injury, associated long bone fractures and those who were treated surgically were found to have significantly longer LOS (P <0.001). Twenty-nine patients died giving an overall mortality rate of 11.2% and it was significantly associated with; the extreme of age, presence of pre-morbid illness and associated extra-cranial injuries, ISS ≥ 16, admission GCS < 9 and SBP < 90mmHg, the duration of loss of consciousness, the need for ICU admission and finding of space occupying lesion in CT scan brain (P < 0.001). The majority of patients (222; 85.4%) had good recovery. Five (1.9%) patients were discharged on request, two (0.8%) patients left against medical advice and the other two (0.8%) patients were referred to higher centre for more expertise neurosurgical treatment. Nine (3.5%) patients had complications related to both head injuries as well as associated extra-cranial injuries. These included neurological deficit in 3 (33.3%), post-traumatic seizures in 3 (33.3%), post-concussion syndrome in 4 (44.4%), cerebral abscess in 2 (22.2%) and complications related to long bone fractures in 5 (55.6%). A total of 62 (23.8%) patients were available for follow up at three month after trauma. Outcome of patients was measured at 3-month after injury using Glasgow Outcome score (GOS) and categorized as “favourable outcome ( GOS grade 4 to 5)” and unfavourable outcome (GOS grade 1 to 3) in 57 (91.9%) and 5 (8.1%) patients respectively. Discussion Globally, head injuries remain an important public health problem and contribute significantly to high morbidity, mortality and long term disability (Sharma et al, 2003; Emejulu & Malomo, 2008). The majority of patients in our study were young adults with males outnumbering females. These findings are comparable with previous studies which reported overall ratios of males to females to range from 3:1 to as high as 11.1:1 (Marik et al, 2002; Sharma et al, 2003; Emejulu & Malomo, 2008; Yattoo & Tabish, 2008; Agrawal et al, 2009). This group represents the economically active age and portrays an economic lost both to the family and the nation and the reason for their high incidence of head injuries reflects their high activity levels and participation in high-risk activities. Male predominance in the present study is due to their increased participation in high-risk activities. The fact that the economically productive age-group were mostly involved demands an urgent public policy response. Road traffic crushes have been reported to be the commonest cause of head injuries in most studies as supported by the present study (Marik et al, 2002; Sharma et al, 2003; Laleef & Abedayo, 2007; Emejulu & Malomo, 2008; Yattoo & Tabish, 2008, Agrawal et al, 2009). This may be attributed to recklessness and negligence of the driver, poor maintenance of vehicles, driving under the influence of alcohol or drugs and complete disregard of traffic laws. The low incidence of helmet use among motorcyclist and passengers in this study reflects increased risks of head injuries in this region (Chalya et al., 2010). Falls has been reported to be the second common cause of head injury in many studies and tends to affect the extreme of age (Vazquez-Barquero et al. 1992; Emejulu & Malomo, 2008, Yattoo & Tabish, 2008, Agrawal et al, 2009,). This is contrary to the present study in which assault was found to be the second common cause of head injuries. Our finding is similar to a study from Glasgow, Scotland which reported assault as the second most common cause after falls (Thornhill et al, 2000). High incidence of head injuries due to assault in this study is likely to be due to high incidence of interpersonal violence and increased criminal activities in this area. In the present study, none of our patients had received any pre-hospital care at the site of injury and majority of them were brought in by relatives, friends, Good Samaritan or by police who are not trained to care for trauma patients. Only five patients were brought in by ambulance. Similar observations have been noted in Kenya and Tanzania (Mang’ombe & Kiboi, 2001; Chalya et al., 2010). The management of patients with head injuries has several important elements: adequate pre-hospital care, rapid transport to a specialized centre, complex in-hospital care and rehabilitation. The prehospital phase of management is the most important interval in determining the ultimate outcome after head injury. The delay in presentation to hospital and the mode, by which patients arrive, shows gaps in the referral system and is clear testimony that pre-hospital care is lacking. The lack of advanced pre-hospital care in our environment coupled with ineffective ambulance system for transportation of patients to hospitals are a major challenges in providing care for trauma patients and have contributed significantly to poor outcome of these patients due to delay in definitive management. Scalp injuries (scalp hematoma, laceration and cut wounds), cerebral concussion and cranial (vault and basilar) fractures were the most common type of head injuries sustained. This is in agreement with finding from other studies (Mwang’ombe & Kiboi, 2001; Sharma et al., 2003; Emejulu & Malomo, 2008). The presence of associated injuries is an important determinant of the final outcome of head injury patients. In the present study, musculoskeletal injuries mainly soft tissue injuries and long bone fractures were the most common associated extra-cranial injuries and significantly influenced the final outcome of our patients. This was in agreement with findings of studies done elsewhere (Mwang’ombe & Kiboi, 2001; Agrawal et al., 2009,). Early recognition and treatment is important in order to reduce mortality and morbidity associated with head injuries. The mortality rate in our study was high in patients with SBP < 90mmHg (72.4%) compared with those with SBP > 90mmHg (27.6%), which is comparable to other reported rates (Mang’ombe & Kiboi, 2001). In our study, the majority of patients had mild head injuries. This is in agreement with other studies (Emejulu & Malomo, 2008; Yattoo & Tabish, 2008). The GCS value at the time of admission is the single most important predictor of outcome of head injury patients as supported by the present study. In the present study, the skull radiography detected abnormal findings in about 42% of patients. Historically, imaging of the head-injured patient relied on skull radiographs. Of recent, studies have shown that the use of skull radiographs in evaluation of patients with head injury is controversial (Masters et al,. 1987). Significant intracranial injuries have been known to occur with normal skull X-ray studies. Because of low sensitivity skull radiograph is useful only for imaging of calvarial fractures, penetrating injuries, and radiopaque foreign bodies (Masters et al, 1987). With the widespread availability and advancement of head CT scanning, the technique has become the diagnostic procedure of choice when evaluating acute head trauma. In the present study, CT scan was more useful in demonstrating the intracranial lesions. Most of our patients were treated conservatively and only few patients underwent surgical treatment, which is in agreement with other similar studies (Mwang’ombe & Kiboi, 2001; Emejulu & Malomo, 2008, Agrawal et al, 2008, Agrawal et al, 2009; Rajendra et al, 2009). The low incidence of surgical treatment in our study is attributable to the high incidence of patients with mild head injuries requiring no surgical intervention. The most common indications for surgical treatment in the present study were surgical l wound debridement for scalp lacerations, elevation of depressed skull fractures, evacuations of intracranial hematomas and treatment of associated extra-cranial injuries. Similar treatment trend was also reported in Nepal (Agrawal et al, 2009). The majority of patients in this study had good recovery which is comparable with other studies (Emejulu & Malomo, 2008, Agrawal et al, 2008, Agrawal et al, 2009, Mwang’ombe & Kiboi, 2001). This observation can be explained by the high incidence of patients with mild head injuries. The complication rate in this study was 3.5%, which is lower than in other series (Mwang’ombe & Kiboi, 2001, Agrawal et al, 2009). The overall LOS for both survivors and non-survivors in our study were found to be higher than that reported by other authors (Mwang’ombe & Kiboi, 2001). This finding can be explained by the large number of patients with long bone fractures which took time to heal as majority of them were treated with either skeletal or skin traction and only few patients were treated with open reduction and internal fixation. Another reason is that patients who had RTAs, penetrating head injuries and those who were treated surgically were found to have longer in-hospital stay contributing significantly to the overall LOS. The mortality rate in the present study was also found to be high than that reported in other studies (Agrawal et al., 2009). However, much higher mortality rates of 19.8%-29% and 56.2% have been reported in Nigeria and Kenya, respectively (Mwang’ombe & Kiboi, 2001; Emejulu & Malomo, 2008). The factors responsible for this findings were the extreme of age, presence of pre-morbid illness and associated extra-cranial injuries, admission GCS < 9 and SBP < 90mmHg, the duration of loss of consciousness, the need for ICU admission and finding of space occupying lesion in the brain. The low level of follow up in our study is comparable with what was reported in Nigeria (Emejulu & Malomo, 2008). This could be due to a preponderance of mild head injuries with good outcome. It could also be due to low complication rate observed in this study. In agreement with other studies (Emejulu & Malomo, 2008; Agrawal et al, 2009), the majority of our patients had favourable outcome at three month duration after trauma. This can also be explained by high incidence of patients with mild injuries and low complication rate in our study population. Irregular availability of CT scan (due to breakdown or inability of patients to afford) and the large number of loss to follow up were the major limitations of this study. However, despite those limitations, the study has provided local data that can be utilized by health care providers to plan for preventive strategies as well as establishment of management guidelines for patients with traumatic head injuries. This information can also be used to guide the future funding of public health programs geared toward prevention. In conclusion, head injury is an important public health problem accounting for a substantial proportion of all trauma admissions at Bugando Medical Centre. RTA continues to be the major etiological factor for head injuries and the commonly affected victims are young adult males in their productive and reproductive age group. Urgent preventive measures targeting at reducing the occurrence of RTAs is necessary to reduce the incidence of head injuries in this region. Acknowledgements The authors are thankful to all those who were involved in the care of the study patients. Special thanks go to all the members of staff of Surgical Department for their stimulating criticisms and contributions they made in the preparation of this manuscript. More sincere and heartfelt appreciations go to Dr. Stephen Mshana for his never ending assistance, encouragement and technical advice rendered since the inception of the idea to the final writing of this manuscript. References
Copyright 2011 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th11012t4.jpg] [th11012f1.jpg] [th11012t3.jpg] [th11012t2.jpg] [th11012t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}