 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
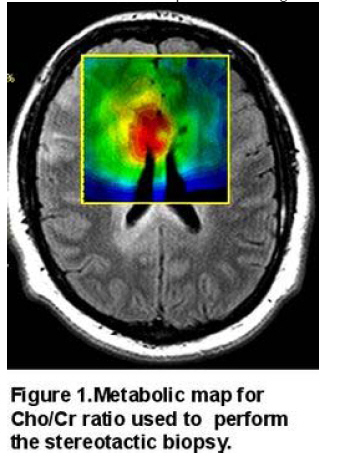
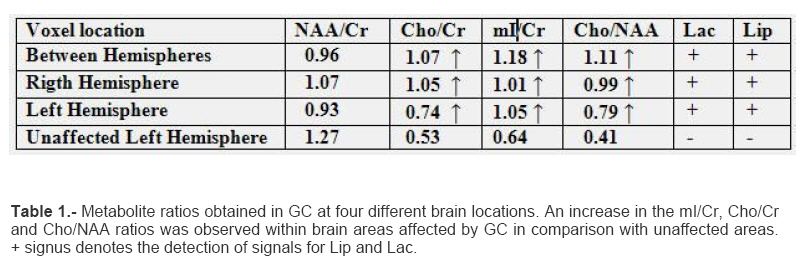
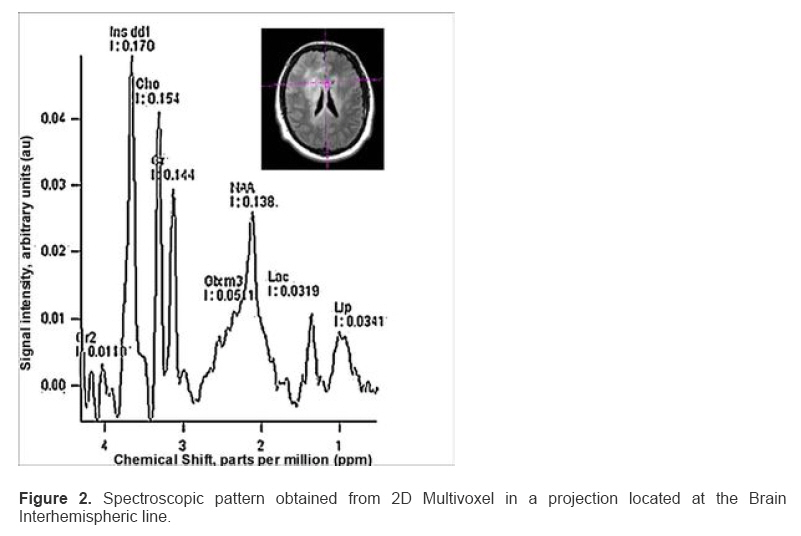
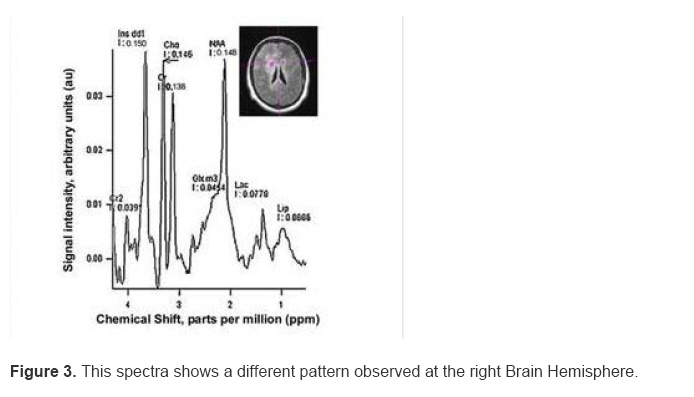
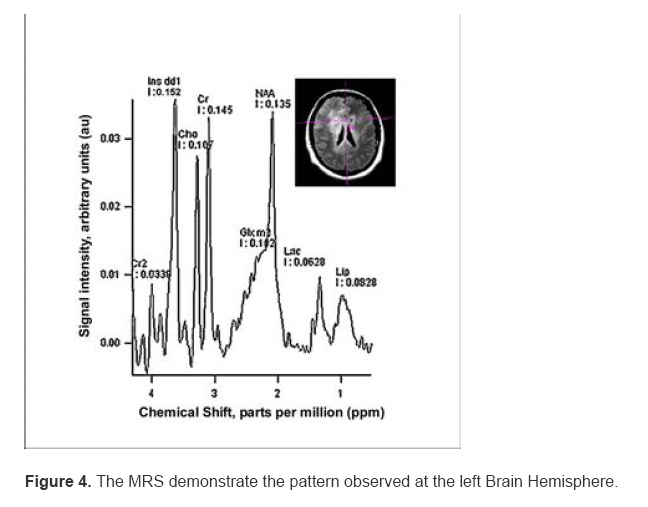
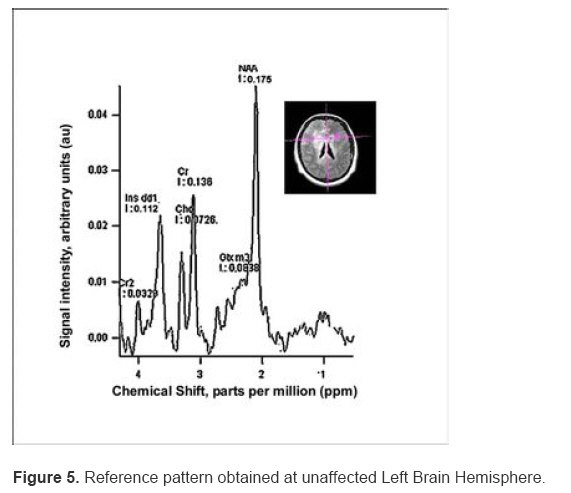
¹H Magnetic Resonance Spectroscopy demonstrates different metabolic features in Gliomatosis Cerebri Espectroscopía de Hidrógeno por Resonancia Magnética muestra diferentes cambios metabólicos en la gliomatosis cerebri Arturo Alvarado 1 , Verónica Velasco 2, Jomer García 3, María Daniela González 4, Belén Torres 5, Amanda Peña 6, Mariangela Alvarado7 1arturoalvaradopisani@gmail.com, Universidad Central de Venezuela, School of Medicine, Institute of Experimental Medicine, Pharmacology and Toxicology Department, Neurospectroscopy Branch. Caracas, Venezuela. Fecha de recepción: 07/03/2009 Fecha de aceptación: 28/03/2009 Code Number: va09006 La Gliomatosis Cerebri se ha descrito como un crecimiento difuso de células neurogliales en áreas amplias del cerebro. La imagen por Resonancia Magnética no reporta hallazgos específicos por lo que el uso de la Espectroscopía ha sido sugerido para realizar un diagnóstico más preciso y caracterizar mejor esta lesión cerebral. Un paciente con diagnóstico probable de Gliomatosis Cerebri fue estudiado luego de obtener su consentimiento informado. Los metabolitos cerebrales conocidos como Lípidos, Lactato, N-Acetilaspartato, Creatina, Colina y mio-Inositol fueron detectados y las proporciones NAA/Cre, Col/Cre, mI/Cre y Col/NAA fueron calculadas. Se observó un incremento en los cocientes mI/Cre, Col/Cre y Col/NAA en las áreas cerebrales afectadas en comparación con las aparentemente no afectadas. Los resultados del presente estudio nos permiten reportar tres patrones espectrales principales: elevación de la proporción mI/Cre, incremento de la relación Col/Cre y presencia de Lactato y Lípidos. Los diferentes perfiles obtenidos utilizando el tiempo de eco corto demuestran que la Espectroscopía de Hidrógeno por Resonancia Magnética constituye una herramienta de interés para explorar las características metabólicas de la Gliomatosis Cerebri pudiendo ser utilizada en un futuro para realizar el seguimiento de los posibles tratamientos a ser aplicados. Palabras Claves: Espectroscopía de Hidrógeno por Resonancia Magnética, Gliomatosis Cerebri, Metabolismo Cerebral. Abstract Gliomatosis Cerebri is recognized as a diffuse overgrowth of neuroglial cells in wide areas of the brain. Magnetic Resonance Imaging findings are not specific and the use of Magnetic Resonance Spectroscopy to make a more precise diagnosis and characterize this type of Brain Tumour been suggested. One patient with suspected Gliomatosis Cerebri was studied after his informed consent was obtained. Brain Metabolites such as Lipids, Lactate, N-Acetylaspartate, Creatine, Choline and myo-Inositol were detected and NAA/Cr, Cho/Cr, mI/Cr and Cho/NAA ratios were calculated. An increase in the mI/Cr, Cho/Cr and Cho/NAA ratios was observed within brain affected areas in comparison with unaffected areas. The results of this study allowed us to report three main spectral patterns: The raise of the mI/Cr ratio, the increase of Cho/Cr ratio and the presence of Lactate and Lipids. The different profiles obtained using short echo time demonstrate that 1H Magnetic Resonance Spectroscopy may provide a useful tool to characterize the metabolic features of Gliomatosis Cerebri and therefore could be used for assessing the intended treatment. Key Word: 1H Magnetic Resonance Spectroscopy, Gliomatosis Cerebri, Brain Metabolism Introduction Gliomatosis Cerebri (GC) was first reported in 1938 by Nevin who described a diffuse overgrowth of neuroglial cells in wide areas of the brain (1). Magnetic Resonance Imaging (MRI) usually shows a diffuse signal intensity abnormality due to the infiltrative process without mass effect, absence of necrosis and lack of contrast enhancement (2). Therefore, MRI findings are not specific and the use of ¹H Magnetic Resonance Spectroscopy (MRS) to diagnose and characterize GC has been proposed (3). The purpose of this work was to identify the metabolic profiles in a case of GC using MRS. Materials and methods One patient with suspected GC was studied after his informed consent was obtained. MR imaging and MRS were performed with a 1.5-T unit (Avanto®, Siemens Medical Systems, Erlangen, Germany). A localizing Sagittal T1-weighted image was obtained, followed by Axial and Coronal T1-weighted. Axial T2-weighted as well as DARK FLUID or FLAIR images were also acquired. The hybrid Multivoxel 2D Chemical Shift Imaging (CSI) technique uses a Point-Resolved Spectroscopy (PRESS) Double Spin Echo scheme for pre-selection of a Volume of Interest (VOI) that is usually defined to include the abnormality as well as normal appearing brain tissue. We use CHESS for water suppression. In order to avoid a contribution to the spectra from fat signals, the VOI was completely enclosed within the brain and positioned at the center of the phaseencoded Field of View (FOV). VOI consists of an 80 mm x 80 mm region placed within a 160 mm x 160 mm FOV on a 10 mm to 20 mm slice. A 16 x 16 phase-encoding matrix gives an 8 x 8 array of spectra in the VOI with a plane resolution of 10 mm x 10 mm. The parameters used were 1500/30/6 (TR/TE/Acquisitions). Other settings included were a Hamming filter, number of sampling points NP = 1024, BW = 1kHz, preparatory scans = 6, delta frequency = -2.7 ppm. Data underwent apodization through a 1.0 Hz Lorentzian filter, Fourier transformation in time and space, and phase correction. Lipids (Lip), Lactate (Lac), N-Acetylaspartate (NAA), Creatine (Cr), Choline (Cho) and myo-Inositol (mI) intensity signals were detected. NAA/Cr, Cho/Cr, mI/Cr and Cho/NAA ratios were calculated. The GC diagnosis was confirmed by a stereotactic biopsy at the area where Cho/Cr ratio reached the highest value which is represented as an intense red area within the metabolic map showed in Figure 1. Results Data for metabolite ratios of GC at both Brain Hemispheres are summarized in Table 1. The different spectroscopic patterns obtained in the GC case are illustrated in Figures 2, 3 , 4 and 5. Figure 2 shows a spectroscopic pattern in which the most prominent intensity signal is represented by the mI pick. The intensity signals for Cho, Cr and NAA are disposed as in another Brain Tumors: Increase in the Cho/Cr ratio, decrease of the NAA/Cr ratio. Signals for Lac and Lip were also observed. MRS performed at long echo time (Te=135 ms) confirms Lac peak as an inverted doublet signal (Data not shown). Figure 3 shows similar spectroscopic profile compared to Figure 2 with an important difference observed in the NAA intensity signal. According with this pattern the gliosis is more evident in voxels located between the two Hemispheres than voxels placed at Right or Left sides of the Brain. Figure 4 shows a robust signal intensity for mI with high peaks for Cho and Cr in this GC case. Figure 5 is extracted from a voxel placed on the left side of the brain in apparently unaffected tissue. We clearly note the expected values for NAA/Cr, Cho/Cr and Cho/NAA ratios. Therefore, the intensity signal of mI peak is higher than Cho suggesting that probably some osmolar changes occurred as an effect of the proximity of the affected tissue. Discussion MRS allowed us to report at least three main patterns in this GC case. The raise of the mI/Cr ratio, the increase or unaffected Cho/Cr ratio and the presence of Lac and Lip in many combination at the GC affected areas conforms the looks of the different spectral patterns. Figure 2 exhibit a totally inverted profile according to Hunter´s angle rule (HA) (HA < −50°) (4) in which the prominent peak is represented by the mI signal. Gliosis and cell proliferation are probably occurring according with the observed evidence. Previous studies have reported an increase of the mI-Gly/Cr ratio in GC (5-7) and in Low Grade Astrocytoma (8). The potential explanations for this increase are not trivial. Some authors have proposed that the high mI concentration observed in Astrocytoma could be consistent with the idea that mI is a marker for astrocytes (9). As for Astrocytoma, a considerable variation of mI in individual cases was observed. It has been recognized that the mI/Cr ratio is significantly greater in Low Grade Astrocytoma than in normal brain, Anaplastic Astrocytoma, and Glioblastoma Multiforme (10). Our GC case resemble similar spectroscopic characteristics than Low Grade Astrocytoma at the voxels located between the two brain hemispheres. The increase of mI/Cr ratio in Low Grade Astrocytomas could be related to another hypothesis which postulates that mI could be taken as a glial marker (11). In Figure 3, the spectra shows similar characteristics than the one present at Figure 2 with the main difference that the intensity signal for NAA is higher and close to the mI signal value. As well as presented in Figure 2, the Figure 3 denotes an elevated value for Cho/Cr ratio. In pathologically proven adult and pediatric brain tumors, higher Cho concentration was correlated with more malignant lesions (12). Also, in malignant Gliomas, higher Cho levels (expressed relative to Cr or NAA) correlated with shorter survival. Based on these and similar studies, the suggestion has been made that higher levels of Cho metabolites are associated with increased rates of membrane synthesis and cell proliferation. Data extracted from Figure 4 allow us to speculate about the heterogeneous nature of the cells present at the GC. The decrease of the Cho/Cr ratio observed in Figure 4 in comparison with Figure 3, probably suggests a less mitotic index for the tumour cells located at the left side in comparison with the ones at right side of the GC lesion. Common findings showed in Figures 2, 3 and 4 were the presence of signals for Lac and Lip. The presence of Lac in Brain Tumors has been attributed to a tumor-specific metabolism with increased anaerobic glycolysis as a result of ischemic compromise probably due to reduced perfusion mostly in solid tumors. Lac is present also in lesions that contain necrotic regions. GC regions explored in our study often include portions of necrotic tissue due to the heterogeneous nature of the lesion. Therefore, Lac signal intensity in tumor spectra must be interpreted carefully and require verification using long echo time as we did in our study. Previous paper has reported Lac in all tumor types. The lowest Lac levels has been observed in Low Grade Choroid Plexus Papilloma and Pineal Germinoma while the prominent levels have been detected in Pilocytic Astrocytoma and Malignant Medulloblastoma (12) . The Lip signal intensity origin is thought to be the mobile lipid molecules as a result of tissue degradation and necrosis and they it be elevated under hypoxic stress prior to necrosis (13). This is more likely to occur in rapidly dividing tumors that outgrow their blood supply such as Glioblastomas that could be display some characteristics of portions of the GC case discussed in this paper. The current GC case is similar to previous published papers (5-7, 14-16). Thus, the different profiles obtained using short echo time demonstrate that MRS may provide a useful tool to characterize the metabolic features of GC and therefore could be used for assessing the future proposed treatments. Further studies are needed to link the elevation of the mI/Cr ratio with the underlying pathophysiology of GC. References
NOTA: Toda la información que se brinda en este artículo es de carácter investigativo y con fines académicos y de actualización para estudiantes y profesionales de la salud. En ningún caso es de carácter general ni sustituye el asesoramiento de un médico. Ante cualquier duda que pueda tener sobre su estado de salud, consulte con su médico o especialista. Copyright 2009 - Centro de Análisis de Imágenes Biomédicas Computarizadas CAIBCO, Instituto de Medicina Tropical – Facultad de Medicina, Universidad Central de Venezuela The following images related to this document are available:Photo images[va09006f5.jpg] [va09006f4.jpg] [va09006t1.jpg] [va09006f2.jpg] [va09006f1.jpg] [va09006f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}