 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 49, No. 1, Jan-March, 2003, pp. 75-77 Adamantinoma of Tibia: A Case of Late Local Recurrence along with Lung Metastases Filippou DK, Papadopoulos V,* Kiparidou E,** Demertzis NT*** Department of Surgery, **Pathology and ***Orthopaedics, Kifissia Oncological
Hospital "Agii Anargiri", GR-14564 Kaliftaki,
Kato Kifissia, Athens and *1st Internal Medicine Department, Democritus
University of Thrace Medical School,
16 Dimitras str., 68100 Alexanrdoupolis, Greece.
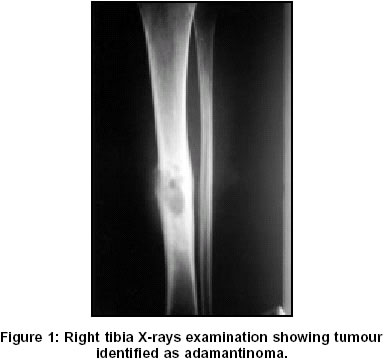
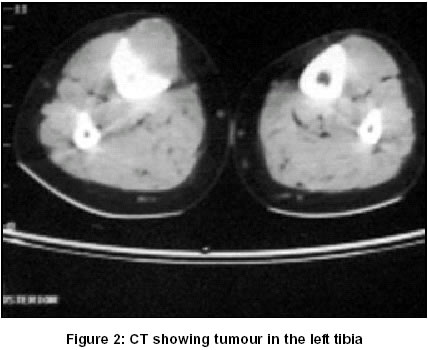
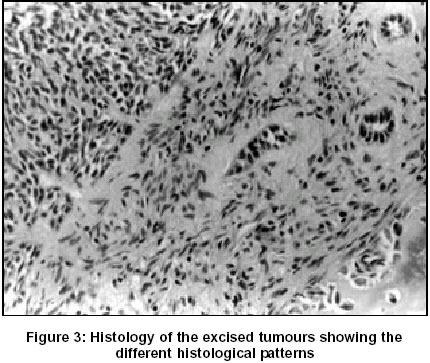
Code Number: jp03015 Abstract: Adamantinomas of long bones are rare primary low-grade malignant tumours composed of cells with epithelial and fibrous characteristics. Local recurrence, though scarce, occurs 5-15 years after the onset of diagnosis. We report a case of local recurrence of an adamantinoma localised in tibia, along with the presence of two lung metastases, 24 years after diagnosis and surgical therapy of the primary tumour. The local recurrence and the lung metastases were removed surgically. The patient remains free of the disease for 3 years. (J Postgrad Med 2003;49:75-77) Key Words: Adamantinoma, tibia, lung metastases, local recurrence. Adamantinomas of the appendicular skeleton, which account for 0.3 to 1% of all malignant bone tumours, are low-grade slow-growing neoplasms probably of mixed mesenchymal and epithelial nature, which develop in the diaphyses and metaphyses of long bones with a predilection for tibia and occasionally fibula. They are usually observed between 20 and 40 years of age and show a predilection for male (male/female ratio 1.3:1, with slightly more aggressive course of disease in males). Pathologically these tumours show a wide range of morphologic patterns, which can mimic many primary or metastatic bone lesions as well as osteofibrous dysplasia, while the true relationship between them still remains to be elucidated.1 The near-benign nature of adamantinoma, in terms of biological aggressiveness, is reflected on the prolonged period of vague symptoms before diagnosis and good survival rates even after the diagnosis of local recurrence or metastases.1,2 Case Report A 42 years old female patient was admitted to the hospital with a swelling on the right tibia. Past history revealed that the patient was operated upon 24 years ago for a pathological fracture of the right tibia and the diagnosis at that time had been adamantinoma. The preoperative radiograph of the right leg showed osteolysis of the bone (Figure 1) and the chest radiograph revealed lung metastases. Regional computed tomography (CT) of the right leg showed that the tumour was invading the surrounding soft tissues. The cortex appeared moderately expanded and attenuated (Figure 2). Bone scanning showed intensive positivity in the middle of the right tibia. The CT scan of the thorax demostrated two lung metastases. One of these was in close contact with the right anterior pulmonary artery and the other was located in the left posterior lobe. Fine needle aspiration (FNA) biopsy confirmed the diagnosis of adamantinoma of right tibia suggesting local recurrence. The patient underwent surgery wherein the tumour was widely resected and the tibia reconstructed with specific recombined osteosynthesis (salvage surgery). The pathological examination of the excised tumour confirmed the diagnosis of adamantinoma set by FNA biopsy (Figure 3). The histological examination revealed a multiforming adamantinoma with basaloid, spindle cellular, and tubular characteristics. Examination of the adamantinoma that had been excised earlier revealed the same characteristics. The post-operative period was without complications and the patient walked in 15 days. The patient underwent two more surgical operations, a right anterior lobectomy of the lung with plastic restoration of the pulmonary artery, and a left posterior lobectomy. Lung infiltration also showed features of adamantinoma. Three years later the patient remains symptom- free of the disease. Discussion This case report refers to an atypical clinical course of an adamantinoma of the tibia. Although lung metastases have been reported in the literature, information concerning the time needed for them evolve is inadequate.3,4 In our case, the local recurrence as well as occurrence of lung metastasis were considerably delayed. The most common symptoms include a slowly evolving swelling (dull pain that is never very intense) and pathologic fractures. . The tumor usually metastasises to the lungs or to the bones. Although uncommon, haemoptysis could be the first symptom to denote lung involvement.5 As far as radiographic features are concerned, the commonest appearance is that of multiple, sharply circumscribed lucent zones of various sizes, with sclerotic bone interspersed between the zones and extending above and below the lucent zones. Sometimes the radiographic aspects of adamantinoma are similar to those of osteofibrous dysplasia of tibia.6 MRI is useful in differentiating between adamantinoma from osteofibrous dysplasia. On plain radiographs, both of them may show polycyclic osteolysis refereed to as soap-bubble appearance. MRI can give information not only on the extent of the tumor, but also about its origin.7 The pathological diagnosis of adamantinoma can be confusing as the appearance of the tumour varies remarkably. More often, a mixture of several patterns is observed in each case. The main histological types are : a. Basaloid type: Cords and islands of cells similar to basal cell carcinoma.
It is not very unusual for more than one type to exist in the same specimen. In our case the tumour showed different patterns and these patterns were found in both tibia and lung. The diagnosis of adamantinoma is difficult due to the rarity and the multiplicity of histological features. The differential diagnoses include epithelial metastasis, hemangioendothelioma, fibrous and osteofibrous dysplasia. In cases of doubt, the diagnosis should be ascertained by the use of FNA.9,10 The surgical procedure included wide resection of the tumor in healthy tissues and salvage surgery, with combined osteosynthesis (screws, acrylic cement in a unique body). This technique offers stability and thus early remobilization of the patient within a mean time of two weeks. This allows the fastest recovery of the patient, needed especially where additional surgical interventions are indicated (e.g. for removal of metastases). The development of late metastases is not unusual in inadequately treated patients. References
Copyright 2003 - Journal of Postgraduate Medicine. Online full-text also available at http://www.jpgmonline.com/ The following images related to this document are available:Photo images[jp03015f3.jpg] [jp03015f2.jpg] [jp03015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}