 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 10, No. 2, 2005, pp. 135-141 Detection of endometrial pinopodes by scanning electron microscopy in hormone-controlled and stimulated cycles Wafaa M. Aboul Enien, M.D.*, Fawzia M. Saleh, M.D.*, Hassan N. Sallam, Ph.D.*, Safinaz H. Safwat, M.D.†, Mervat A. Mohamed * Department of Obstetrics and Gynecology
and Department of Histology, Faculty of Medicine, Alexandria University, Egypt. Received November 29, 2004; revised and accepted March 10, 2005 Code Number: mf05025 ABSTRACT Objective: To assess the effects of clomiphene
citrate (CC) and combined oral contraceptive pills (COP) on endometrial pinopode
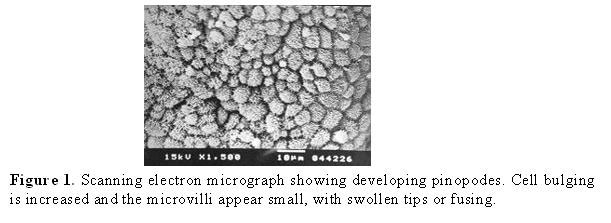
expression. Keywords:Endometrium, pinopodes, clomiphene citrate, combined oral contraceptive pills, scanning electron microscopy. The term implantation is applied to a series of events initiated by fertilization of ovum that ultimately lead to embedding of blastocyst in the endometrium (1). Implantation of human blastocyst is divided into three phases. In phase I, the blastocyst is free within the endometrial cavity and does not interact with the surface epithelium. In phase II, the blastocyst adheres and then penetrates the surface epithelium and subsequently the underlying stroma. Placentation is the predominant feature of phase III (2). Successful implantation is the outcome of interaction of a receptive endometrium with an intrusive blastocyst. The endometrium is well prepared for implantation during a defined period called the implantation window which is confined to the post-ovulatory days 5-7 of the normal menstrual cycle (3). This short phase of receptivity is preceded by a pre-receptive neutral state and followed by a refractory state of non-receptivity (4). Various architectural, cellular and molecular events in the endometrium are coordinated with the implantation window. These include the formation of pinopodes (5), as well as, changes in the expression of adhesion molecules (6), cytokines and other endometrial proteins (7). Pinopodes are hormone-dependent bleb-like protrusions of the endometrial apical plasma membrane that mediate the epithelial uptake of fluids (pinocytosis) and macromolecules (endocytosis). Fully developed pinopodes exhibit a smooth regular surface that facilitate a close contact between the plasma membranes of the epithelial and trophoectoderm cells (8). Pinopodes are identified with both light and electron microscopy and have been proposed as indicators of endometrial receptivity in humans (9). In normal cycling women, the mid-cycle LH surge is considered luteal day 0. In the early secretory phase (luteal days 1-4), pinopodes are not observed and the endometrial surface shows a distinctive ultrastructure, characterized by tufting and clustering of microvilli. Distinctive changes begin on luteal days 5-6, with thinning and bulging of non-ciliated cells marking the early development of pinopodes or uterodome formation (10). Classic fully developed pinopodes are not common until luteal day 8, when more substantial and readily recognized dome-like structures emerge. Pinopodes then develop a deflated appearance that becomes more obvious as the secretory phase comes to a close (11). Formation of pinopodes is strictly dependent on progesterone, whereas estrogen induces their regression (12). Controlled ovarian hyperstimulation does not affect endometrial pinopode formation in terms of quantity and life span. The cycle days when pinopodes form are specific to the individual, being on average 1-2 days earlier than in natural cycles (13,14). The advanced endometrial maturation may reflect shifts in the window of receptivity, resulting in ovo-endometrial asynchrony and limiting implantation success in stimulated cycles (15). However, in oocyte recipients treated with estradiol and progesterone in hormone controlled cycles, the opening and closure of the implantation window, as indicated by pinopode formation, seems to be delayed (16). The extra time might allow more embryos to develop to the hatched blastocyst stage before closure of the implantation window, and by that means increase conception rates (17). The correlation of pinopode expression with embryo implantation after embryo transfer suggests that pinopodes are good indicators of endometrial receptivity. Furthermore, the preference of human blastocyts to attach to pinopode-presenting endometrial cells in vitro supports this hypothesis (18). However, it remains to be elucidated what function pinopodes have during implantation. Ultrastructure studies indicate that the pinopode presenting apical plasma membrane does not participate directly in embryo-endometrial interactions (17). Pinopode formation is accompanied by loosening of endometrial interepithelial cell contacts that might facilitate blastocyst attachment and penetration. Another possibility may be that the smooth apical plasma membrane on pinopodes allows the presentation of specific receptors as IL-1 receptor type 1, integrin subunit B3 and glutaredoxin which are believed to participate in embryo-endometrial interactions during implantation (19,20). The aim of the current study was to assess the expression of endometrial pinopodes by scanning electron microscopy in hormone-controlled and stimulated cycles. Table 1. Comparison between the clinical characteristics of the three studied groups.
MATERIALS AND METHODS Thirty healthy fertile volunteers aged 20-35 years were recruited from the Gynecology Outpatient Clinic, Department of Obstetrics and Gynecology, El-ShatbyUniversityHospital, Alexandria. All subjects had regular menstrual cycles (25-35 days), had not received exogenous hormones or used an intrauterine device for at least 3 cycles prior to the study and had at least one successful pregnancy. No woman had an abortion or delivery within 1 year before the study. Subjects fulfilling the criteria were randomly divided into three groups: Group I: (n= 10) received steroid hormonal contraception in the form of Nordette tablets (levonorgestrel 0.15 mg and ethinyl estradiol 0.03 mg) during the sampling cycle. Group II: (n=10) received ovarian stimulation with clomiphene citrate (50 mg) starting on the fifth day of the cycle in a dose of two tablets/day for five consecutive days. The control group (group III) did not receive any medication Volunteers were screened for endocrine normality with serum determinations of LH, FSH and E2 on day 3 of the cycle in which the study was performed. Transvaginal ultrasound was also performed on that day to ensure ovarian normality. Table 2. Appearance of endometrial pinopodes in group I. (a)
(One) Pinopodes: developing (D), Fully developed
(F), regressing (R), Microvilli (MV). They all signed an informed consent and were advised to refrain from sexual intercourse or use a barrier contraception during the month of investigation. Moreover, subjects in group II and III were required to start a basal temperature chart (BTC) as a general orientation tool to the cycle. They were also monitored in the periovulatory period with transvaginal ultrasound starting on day 11 for follicle size and endometrial pattern. Endometrial biopsies were obtained without anesthesia as an outpatient procedure using a Pipelle de Cornier (suction curettage). Each volunteer was sampled on days 17,20 and 22 of the cycle. Samples were obtained from the anterior and posterior aspects of the uterine fundus. Each sample was immediately fixed in a solution of 2.5% glutaraldehyde, 0.5% paraformaldehyde, 0.1 mol/L sucrose, 0.1 mol/L sodium cacodylate and 3 mmol/L calcium chloride (pH 7.4), then processed at the Faculty of Science, Alexandria University for scanning electron microscopy. Samples were washed in phosphate buffered saline (pH 7.4), the fixative added with continuous agitation and the suspension left at 4oC overnight. Endometrial tissues were separated from the fixative by a centrifugal separator (1500 rpm) and the supernatant discarded. Precipitated tissues were then dehydrated in a graded series of ethanol dilutions (50%, 70%, 90%, 95%, 100%) for 10 minutes each. The free tissues were suspended in 10% alcohol and the suspension dropped from a pipette onto a glass slide and rapidly dried in a steam of hot air (45o C). Finally, the samples were mounted on the specimen holder, coated with gold to enhance the structural features then examined by a single operator in a blinded manner using a scanning electron microscopy (21,22). Multiple fields were examined as the endometrium may show variable morphology from one area to another. Pinopodes were defined as smooth apical protrusions from the surface epithelium without microvilli and were scored according to the stage of development (developing, fully developed and regressing). RESULTS The clinical characteristics of the three studied groups are shown in Table 1. There was no significant difference between groups as regards the menstrual cycle length (p= 0.823), age (p= 0.796) or body mass index (p= 0.673). Table 3. Appearance of endometrial pinopodes in group II(a)
(One) Pinopodes: developing (D), fully developed
(F), regressing (R), microvilli (MV). Ninety endometrial biopsies were sampled from the thirty volunteers and examined under the SEM. Table 2 summarizes the appearance of endometrial pinopodes in group I. Day 17 revealed no pinopodes, one sample on day 20 had developing pinopodes whereas on day 22, five had developing pinopodes, four had fully developed pinopodes and one had regressing pinopodes. Table 4. Appearance of endometrial pinopodes in group III.(a)
(Three) Pinopodes: developing (D), fully
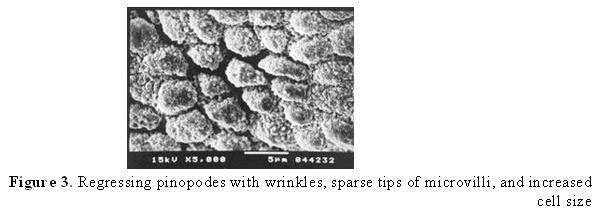
developed (F), regressing (R), microvilli (MV). Table 3 summarizes the appearance of pinopodes in group II. On day 17, three had fully developed pinopodes and six had developing pinopodes. On day 20 and 22, all samples had regressing pinopodes except one that had fully developed pinopodes on day 20. Table 4 summarizes the appearance of pinopodes in the control group. No pinopodes were observed on day 17, whereas, on day 20, six had fully developed pinopodes and four had developing pinopodes. All samples on day 22 showed regressing pinopodes. On comparing the mean day for expression of fully developed pinopodes in the three groups, it was shown that it was significantly accelerated in group II compared to controls (17.9±0.9 and 20.4±0.5 day respectively) and significantly retarded in group I compared to controls (22.4±0.7 and 20.4±0.5 day respectively). Developing, fully developed and regressing pinopodes are shown in Figures 1,2 and 3. DISCUSSION How embryos attach and implant remains a mystery. Implantation represents the remarkable synchronization between the development of the embryo and the differentiation of the endometrium. The endometrium acquires the ability to implant a hatched blastocyst only within a specific time termed the receptive phase (23). An interesting approach to define specific criteria for a receptive endometrium appears to be morphological studies using the scanning electron microscopy. At the time of implantation, the apical membranes of the epithelial cells lining the uterine cavity lose their microvilli and develop large and smooth membrane projections named pinopodes. Their development coincides strictly with the implantation window (24). In the current study, fully developed pinopodes existed in only one endometrial sample in each woman. This indicates that pinopodes have a limited life span and that fully developed pinopodes may only appear for a single day. This is in accordance with previous studies (25,26). However, Acosta et al (27) reported somewhat different results stating that, in some patients, fully developed pinopodes were seen in two endometrial samples spanning a 7-day period. Stavreus-Evers et al (26) commented on the results of the latter study stating that the projections found late in the cycle differ in shape from pinopodes and are probably due to apoptotic processes in the endometrium that precede menstruation. Moreover, contradictory results were also reported by Usadi et al (10) stating that recognizable relatively small pinopodes appear on luteal day five. Classic fully developed pinopodes are observed on luteal day eight and remain clearly evident through luteal day ten. Thereafter, many pinopodes develop a wrinkled appearance suggesting regression before eventual collapse as the secretory phase comes to an end. The latter observations did not invalidate the potential utility of pinopodes as markers of endometrial receptivity. Instead, it was suggested that the morphology of pinopodes rather than their mere presence may be useful in this regard. In the current study, pinopode expression was delayed under the effect of combined oral contraceptive pills. Similar results were reported by Massai et al. (28), Nikas et al. (16) and Psychoyos (29). These results indicate the dependence of the timing of the implantation window as marked by pinopode expression on hormonally regulated factors. However, in a recent study by Oborna et al. (30) it was suggested that hormonal preparation of the endometrium do not change the timing of pinopode expression compared to natural cycles. Our observations revealed accelerated endometrial differentiation and early appearance of pinopodes in patients who received clomiphene citrate compared to controls. This agrees with previous studies (12,15,31-33). However, the discrepancy between different studies as regards the day of appearance of fully developed pinopodes may be due to differences in the stimulation protocols used or the inclusion as pinopodes of small apical uterine folds during the early luteal phase. Moreover, in some protocols, patients were not biopsied sequentially or even after day 19 which might have obscured the progressive changes in pinopode expression. The premature expression of pinopodes is in line with the observation of precocious luteal transformation following ovarian stimulation, however the clinical relevance with respect to the establishment of a clinical pregnancy awaits further validation (32). In the current study, the timing of appearance of fully developed pinopodes showed individual variations among patients in the same group and receiving an identical hormonal treatment. This is in accordance with previous word (34-35). Hence, it is necessary in clinical practice to predict the timing of nidation window on individual basis. The detection of uterine pinopodes during a pre-replacement cycle could be a valuable tool allowing estimation of the optimal date for successful embryo transfer in IVF (15). Regarding some concerns about the reliability of microscopic findings after sequential sampling, SEM is a suitable method to address this question. SEM can view the entire surface of the specimen and very often the sites of previous sampling are visible as gaps surrounded by regenerating epithelium. Such areas tend to localize at the edge of the biopsy pieces and the rest of the tissue looks perfectly normal, in terms of epithelial integrity and evolution, including pinopode formation. Therefore, sequential endometrial sampling provides reliable material for SEM studies. In conclusion, our study reveals that the cycle days when pinopodes form are specific to the individual being on average 1-2 days earlier in ovarian stimulation and retarded in hormone controlled cycles compared to natural cycles. These changes in pinopode expression may reflect shifts in the window of receptivity, resulting in ovo-endometrial asynchrony and hence in suboptimal implantation rates. REFERENCES
© Copyright 2005 - Middle East Fertility Society The following images related to this document are available:Photo images[mf05025f3.jpg] [mf05025f1.jpg] [mf05025f2.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}