 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
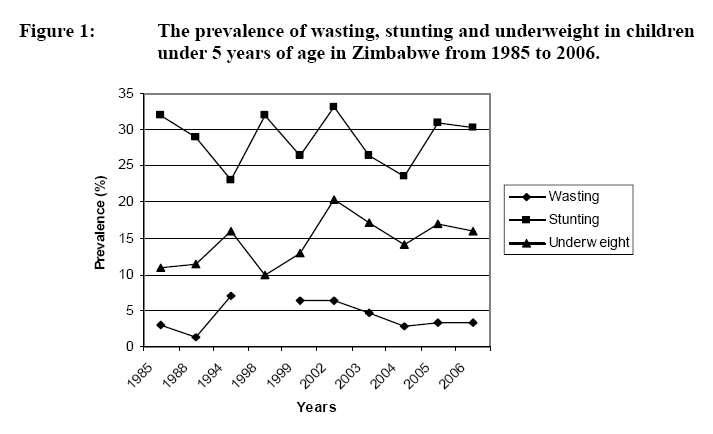
African Journal of Food Agriculture Nutrition and Development, Vol. 9, No. 1, Jan, 2009, pp. 502-522 Status of Micronutrient Nutrition in Zimbabwe: A Review Gadaga TH1*, Madzima R2 and N Nembaware3 * Corresponding author: Email: tgadaga@hotmail.com Code Number: nd09003 ABSTRACT More than 65% of the Zimbabwean population live in the rural areas and are food insecure especially due to droughts. The population experiences fluctuating levels of malnutrition including vitamin and mineral malnutrition. This paper constitutes a review of the micronutrient malnutrition status of the Zimbabwean population, focusing on the period from 1980 to 2006, using data from nutrition surveys, the demographic health surveys, sentinel surveillance and monitoring programmes. Data collated from the numerous surveys show that a significant proportion of children under 5 years of age, school children, pregnant and lactating women experience malnutrition. In 1999, 35.8% of children 12-71 months of age were vitamin A deficient (serum retinol <0.70µmol/L). In March 2005, 22.3% of targeted children received vitamin A capsules during routine visits to clinics for growth monitoring and immunisation. However, about 82% of the targeted children received vitamin A capsules during Child Health Days, which is therefore an effective strategy. More than 95% of households in the country have access to iodised salt, while the median urinary iodine in 2005 was about 200µg/L. In 1997, about 9% of the population were found to have less than 10µg/L serum ferritin leading to the conclusion that iron deficiency anaemia was of public health significance in Zimbabwe. About 31% of women of child bearing age were found to be anaemic in a 1999 survey leading to the expansion of iron tablet distribution during ante-natal visits. However, in 2005, 43% of pregnant women were taking iron supplements during pregnancy, with women in urban areas less likely to take iron supplements than women living in rural areas. There is need, therefore, to increase efforts to reduce micronutrient deficiencies in the country. Fortification of vegetable oil with vitamin A is technically feasible and the vitamin is stable for up to 6 months at 23oC. With increasing evidence of other micronutrient deficiencies such as the B-group vitamins, fortification of staple foods, such maize meal, could be a long term strategy of addressing micronutrient deficiencies in Zimbabwe. Key words: Micronutrients, malnutrition, vitamin A, anaemia INTRODUCTION Micronutrient deficiencies impact negatively on the social, economic and intellectual development of individuals and communities. According to the Global Progress Report on Vitamin and Mineral deficiency, more than half of the population in Africa, including many who consume sufficient calories and protein, lack critical vitamins and minerals [1]. An estimated 350 million women and children in Africa suffer from deficiencies in iron, vitamin A and folic acid. The WHO estimates that deficiencies in iron, vitamin A and zinc each rank among the top 10 leading causes of death in developing countries through disease [2]. Unfortunately, most people affected by micronutrient deficiencies do not show overt clinical symptoms, nor are they themselves aware of the deficiency, a phenomenon called “hidden hunger” [3]. At the World Summit for Children (1990), world leaders adopted a Declaration on the Survival, Protection and Development of Children and a Plan of Action for implementing the Declaration in the 1990s. There was agreement on the need for the reduction in severe, as well as moderate malnutrition among children under-5 years of age by half of the 1990 levels, to reduce iron deficiency anaemia in women by one third of the 1990 levels, virtually eliminate iodine deficiency disorders, and virtually eliminate vitamin A deficiency and its consequences, including blindness [4]. The International Conference on Nutrition (1992) and the United Nations General Assembly (2002) sought further commitment to sustainable elimination of iodine deficiency disorder by 2005 and vitamin A deficiency by 2010, reduce by one third the prevalence of anaemia, including iron deficiency anaemia by 2010, and accelerate programs towards reduction of other micronutrient deficiencies through food fortification and supplementation. Over the past 40 years many developed countries have dealt with the problem of vitamin and mineral deficiency (VMD) through fortification, supplementation, dietary diversification, education and disease control. These are practical and affordable solutions that developing countries can adopt for the benefit of their populations. A World Bank Review of micronutrient deficiencies in Zimbabwe showed that there were recorded incidences of vitamin and mineral deficiencies at health institutions [5]. Recent survey data also showed that vitamin and mineral deficiencies still remain problems of public health significance in the country. This report reviews progress made in addressing micronutrient deficiencies in Zimbabwe, focusing on the period 1980 to 2006. OVERVIEW OF NUTRITION SITUATION IN ZIMBABWE Over the years, information on the nutritional status of Zimbabweans has been collected in various national surveys and through child growth monitoring data recorded at health centres and stored in the National Health Information System (NHIS). The Zimbabwe Demographic Health Surveys (ZDHS) and Zimbabwe Vulnerability Assessment (ZimVAC), as well as the Food and Nutrition Surveillance (FNS) and the IDD Sentinel surveillance are important sources of nutrition information for decision makers. The ZDHS surveys were initiated in 1988, and subsequently done in 1994, 1999, and 2005 [6]. Initially, the ZDHS only reported on the protein-energy nutrition status of children in the age group 6 – 59 months, namely, prevalence of stunting, wasting and weight for age, as well as breastfeeding practices. In 1999, ZDHS included several questions to evaluate the micronutrient status of women and children. As shown in Figure 1, the nutrition situation of the population has been constantly changing. The people living in drought prone districts in the southern parts of the country, namely Matebeleland South, Matebeleland North and Masvingo, are most vulnerable to under nutrition. The lack of adequate food intake in general is a major contributing factor in vitamin and mineral deficiencies, especially iron and vitamin A [7. In other words, populations that are malnourished are most likely vitamin and mineral deficient, and malnutrition will generally indicate food insecurity [8] IODINE DEFICIENCY DISORDERS (IDD) Lack of sufficient intake of iodine in the diet causes the thyroid gland to enlarge resulting in goitre. However, goitre is only one of the indicators of IDD. Many disorders begin before birth and persist throughout the life cycle. Infants born to iodine deficient women, if they survive, may be cretins with short life expectancy, physically or mentally retarded, deaf or mute and spastic, depending on degree of iodine deficiency. It is estimated that globally, about 655 million people have goitre, while some 43 million are affected by some degree of mental impairment of which 6 million are cretins [9]. Goitre has long been recognized by indigenous Zimbabweans and a number of words for the condition in local languages exist. In a study done in 1968 in the Chikwaka area of Goromonzi district, a prevalence of up to 75% endemic goitre was reported. More than half of those affected had visibly enlarged thyroids [10]. Around the same time, up to 45% total goitre rate (TGR) and 6.6% visible goitre rate (VGR) were reported for Omay in Kariba district [11]. The goitre prevalence in 1986 was to some extent similar to what was reported in 1968. A survey of 188 schoolchildren in Chinamhora communal lands reported a TGR of 44%, while in Wedza district the TGR was 73% [12, 13]. However, it was the national goitre survey of 1988 that highlighted iodine deficiency to be of public health significance in Zimbabwe. The survey showed that TGR in Zimbabwe ranged between 10.8% in Harare and 78.7% in Murehwa district (Table 1), with the prevalence varying from moderate to severe. Twenty of the 50 districts surveyed had goitre prevalence rates of more than 50%. The TGR for the provinces varied from 17% in Matebeleland South to 52% in Mashonaland Central. According to these results, every province in the country could be classified as suffering from at least a mild level of endemic goitre, with Murehwa district the most affected. Table 1: The prevalence of goitre in Zimbabwe in after the 1988 National Goitre survey
UNIVERSAL SALT IODISATION A national inter-sectoral committee on iodine deficiency disorders (IDD) was set up in 1989 with its terms of reference, among others, to monitor the implementation of an IDD plan of action and facilitate the enacting of legislation for the control of IDD. The committee came up with a national plan of action in 1991, with the objective of eliminating iodine deficiency disorders by the year 2000. It recommended universal salt iodisation (USI) as the main strategy, while distribution of iodised oil capsules was suggested as an interim strategy in severely affected areas. In 1992, universal salt iodisation was adopted but the legislation was only put in place in 1995. The Food and Food Standards (Condiments) (Amendment) Regulations, 1995 (Statutory Instrument 69 of 1995) set the iodisation level at between 30 and 90 mg/kg (ppm). Following reported cases of hyperthyroidism, this regulation was amended and replaced by the Food and Food Standards (Condiments) (Amendment) Regulations, 2000 (Statutory Instrument 44 of 2000), which now requires that all salt manufactured or sold for human consumption in Zimbabwe, including crude salt, table salt, flavoured salt or in other forms, shall be iodised with potassium or sodium iodate and contain the equivalent of not less than 25mg or more than 55 mg of iodine per kilogram of salt. Universal salt iodisation (USI) was successful in Zimbabwe mainly because virtually all of the country’s salt requirements were imported with very insignificant local small-scale production. The quality of the imported salt could be easily monitored. By 1994 only eight companies handled almost 80% of all salt imports with the bulk of the salt coming from Botswana. Salt was sold to consumers packed in 0.5, 1 and 2 kg bags. However, the number of salt traders/importers has since increased, with some of the new players not aware of the IDD control programme. Some importers have been suspected of bringing in inappropriately iodised salt. Although there are some areas in Zimbabwe with potential salt deposits such as the Hot Springs, Gonarezhou National Park, Zambezi Basin and Chipinge, the deposits are insignificant for commercial exploitation. The local deposits are mostly utilized for household consumption and very little if any, is sold commercially. PROGRESS IN ELIMINATING IDD Since the introduction of USI there have been significant changes in the iodine status of the population as shown by the decrease in prevalence of visible and palpable goitre. For example, in 1996, the TGR in Chinamora district, determined by palpation in primary school children (n=329) of both sexes aged 6–14 years, was found to be 9%. Before the introduction of USI this rate was 44%. The median urinary iodine level was about 450μg/L, double the upper limit of normal [14]. Only 5% of the samples were below 100μg/L. In 1999, a National Micronutrient survey was conducted which showed that 97.8% of households in Zimbabwe were consuming iodised salt. Urine iodine levels of primary schoolchildren showed that only 8.5% had <100μg/L, indicating a normalization of iodine nutrition in the population [15]. Unfortunately, at that time, several cases of hyperthyroidism were reported that indicated excess iodine in the diet [16]. About 12 deaths solely due to thyrotoxicosis were reported at Parirenyatwa Hospital in Harare between 1993 and 1995 [16]. It was then suggested that the quality of iodised salt should be constantly monitored. The level of iodisation which had initially been recommended at 30–90 mg/kg was revised to 25-55mg/kg. The Ministry of Health and Child Welfare, through the Environmental Health officers now continuously monitors the IDD situation in the country by routine sampling of salt at retail level, and through biannual IDD sentinel surveillance in 12 districts of the country. The IDD sentinel surveillance is regularly conducted in 12 districts: Harare, Bulawayo, Chitungwiza, Nyanga, Chimanimani, Centenary, Murehwa, Matobo, Shurugwi, Chegutu, Bikita and Binga. In each district 3 schools are chosen at random and in each of these schools about 50 pupils are chosen using systematic random sampling for collection of spot urine specimens. Goitre surveys are conducted at the same time. Salt samples for titration are also collected from households (brought by schoolchildren) and retail outlets in the catchment area of the 3 schools. The first such surveillance was done in 1992. However, the surveys have not been held biannually as scheduled and after 1992, the surveys were only done in 2002 and then in 2005. In the 2005 IDD sentinel surveillance exercise, more than 1800 salt samples were tested for iodine. About 54% of the iodised samples had levels of iodine within the recommended range of 25-55 mg/kg. Another 39% of the samples had iodine levels below 25 mg/kg and the remaining 7% had levels above 55 mg/kg (Table 2). Binga had the highest proportion of salt with iodine levels in the recommended range, probably indicating a uniform source for their salt. In total, 99.7% of the salt samples tested contained iodine. Table 2: The level of iodisation of salt samples collected from retail outlets during the 2005 IDD sentinel surveillance
Source: IDD Sentinel Site Surveillance, May 2005. *NA = Not Available Iodine deficiency disorders monitoring was also integrated into the Food and Nutrition Surveillance (FNS) programme. However, some of the districts among the 10 sentinel districts used during FNS are different from those of the IDD sentinel surveillance (Table 3), and therefore results may not be directly comparable. From the November 2004 Food and Nutrition Surveillance data, 90% of households interviewed used iodised salt, while about 7% were using un-iodised salt. About 3% had no salt at all at the time of sampling (Table 3). Centenary district had the highest number of households with un-iodised salt and also those without salt at the time of sampling. By comparison, in June 2005 Zimbabwe Vulnerability Assessment Committee (ZimVAC) reported that on average 95% of households were using iodised salt. However, sub-optimal levels of iodine were detected in some salt samples. Mashonaland East, Masvingo, Mashonaland West, Midlands and Matebeleland South had 25%, 24%, 16%, 11% and 3% of the households, respectively, using un-iodised salt, indicating that the IDD monitoring programme needed strengthening. The results also suggest that some communities in the country could be having access to salt obtained from other sources other than Botswana Ash and other recommended suppliers. Centenary (67% iodised salt), Bulilimamangwe (80.2%), Kwekwe (85.7%) and Kariba (86.7%) seem to be worst affected [17]. Table 3: The use of iodised salt at household level in 10 sentinel districts in Zimbabwe according to the 2005 Food and Nutrition Surveillance programme
Urine iodine levels also confirm that there has been a reduction in IDD prevalence in Zimbabwe (Table 4). In 1992 urinary iodine levels in schoolchildren were well below 100µg/L but a sharp rise in urinary iodine levels was observed in a few districts in 1993. A further increase was noted in 1995 with quite a number of districts recording urine iodine levels above 300µg/L, which coincided with the time iodine induced hyperthyroidism (IIH) was observed in some parts of the country. The urine iodine levels showed a major reduction from the 1995 highest levels of 600 μg/L to 220 μg/L in 2005, indicating a stabilization of the iodine intake in the population. However, in Nkayi and Shurugwi districts the median urinary iodine levels were still above 600µg/L in 2005. The observed reduction could be linked to the amendment of the Food Regulations in 2000. As the IDD prevention programme progresses, goitre rates become less useful indicators and urinary iodine level progressively becomes the elimination criteria. [14]. Table 4: Changes in median urinary iodine concentration after introduction of universal salt iodisation in Zimbabwe
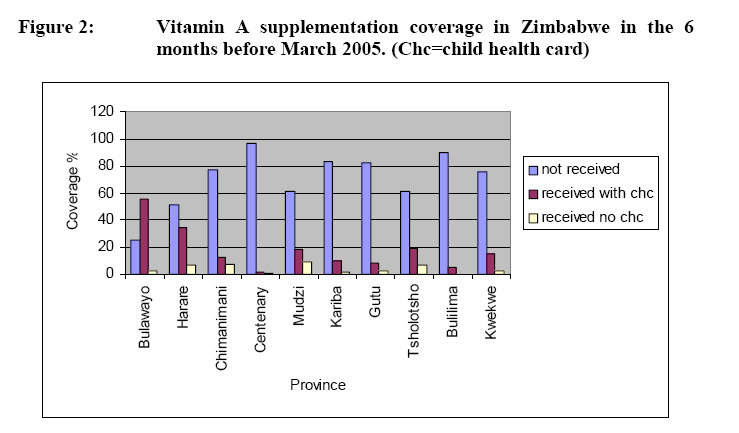
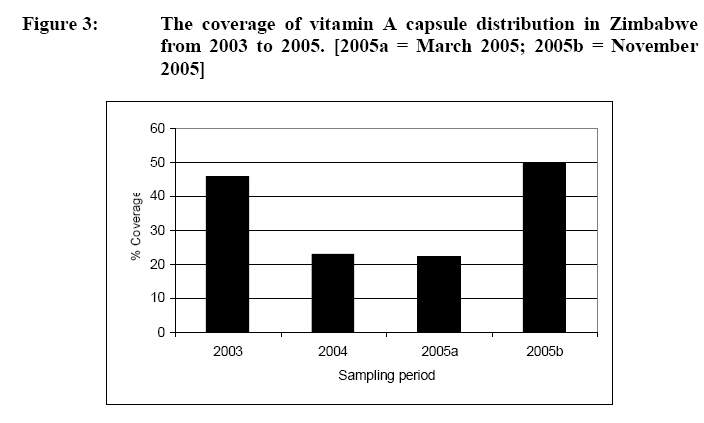
Vitamin A deficiency (VAD) can lead to visual malfunctions such as night blindness and xerophthalmia and can reduce immune responsiveness causing increased incidence and severity of respiratory infections, gastrointestinal infections and measles. Vitamin A deficiency is not only the cause of childhood blindness across developing countries, its effects on children’s immune system directly results in around 10.8 million deaths each year. According to UNICEF, eradicating VAD would cut child deaths due to measles by 50% [17]. Maternal VAD may contribute to mother to child transmission of HIV and contribute to increased infant mortality [18]. Vitamin A can be obtained from food either as preformed vitamin A in animal products or as provitamin A carotenoids, for example a-carotene, β-carotene and β-cryptoxanthin in plant products. Prior to 1999, the vitamin A deficiency status in Zimbabwe was not completely known except for a few limited studies. For example, McManus investigated about 250 cases of xerophthalmia in rural Matebeleland North and South [19]. Most of these cases were observed following measles infection, while some were associated with protein energy malnutrition (PEM) and some with dysentery. Most cases were seen from May to December when milk is less available and green vegetables are consumed dry. In a separate study, Decker studied 988 cases of hospitalized children in Lupane and found that ocular lesions from measles were much more severe among black children with low vitamin A intake [20]. However, in 1983, findings from the World Bank Population Health and Nutrition Sector review seemed to indicate that vitamin A deficiency was uncommon in Zimbabwe [5]. A study conducted in Matebeleland North in 1991 recorded the prevalence of Bitot’s spots at 0.17% and that of vitamin A related corneal scars at 0.03%, well below the 0.5% WHO criteria for VAD of public health significance [21]. The National Micronutrient Survey, however, showed a more detailed picture of the vitamin A deficiency prevalence in Zimbabwe [15]. The survey showed that 35.8% (n=346) of children 12-71 months had vitamin A deficiency, with serum retinol levels below 0.70mmol/L. Among schoolchildren of 6-14 years age group VAD prevalence was 18% (n=657). In women of child bearing age, 15-49years, VAD prevalence was 6.9% (n=804) [15]. At the same time, however, the ZDHS (1999) showed that 3 in 4 children under 3 years of age received food rich in vitamin A. Unfortunately the types of foods given were not recorded [6]. All this information pointed to the need for Zimbabwe to take measures to adequately and continuously address VAD in the population. Several approaches are documented in literature including distribution of high dose oral supplements, food fortification, and education to increase the consumption of foods naturally rich in vitamin A [22]. Zimbabwe has been pursuing all three strategies with different results to date. Targeted vitamin A capsule distribution in Zimbabwe was initiated through UNICEF funding in 2002 and was integrated with the Expanded Programme on Immunisation (EPI) in the same year. In the programme, vitamin A capsules are given to children under 5 years of age every 6 months. The vitamin A capsules were also distributed in areas severely affected by the drought in 2002/2003. The National Nutrition and EPI Survey done in 2003 found that the vitamin A capsules distributed through the routine EPI programme only reached 46% of the targeted population in the country. In November 2004, the Food and Nutrition Surveillance observed that 23% of the children assessed had received vitamin A in the previous 6 months, while 69% had not, and the status of 8% of them was not known [23]. Vitamin A capsule distribution coverage was particularly low in Centenary, Mudzi, Kariba, Gutu, Tsholotsho, Bulilimamangwe and Kwekwe, the worst affected being Centenary (94% without) and Kariba (90%). In the 12-23 and 24-59 months age groups, over 60% had not received vitamin A in the previous 6 months. Among the 10 provinces, Bulawayo had the best coverage of about 40% (verified by a Health card). In March 2005, the vitamin A supplementation coverage had further decreased compared to November 2004 [23]. During this time an average 22.3% of the children in the sentinel districts had received vitamin A, 70.5% had not received while the status of 7% was not known. However, Bulawayo still had the best coverage with over 50% of children having received vitamin A and verified with a health card. Again Centenary (96.9%), Bulilimamangwe (89.8%), Gutu (81.9%) and Kariba (83.4%) had the highest number of children who had not received vitamin A in the previous 6 months (Figure 2). These districts are therefore a cause for concern. The highest number of children (9.2%) who had received vitamin A without documentation was from Mudzi. In November 2005, the third FNS reported that an average of more than 50% of the children assessed had received vitamin A in the previous 6 months and this was verifiable by child health card. About 12% received vitamin A supplementation but it was not recorded in the child health card, while 33.5% did not receive vitamin A supplementation at all. This was an improvement over the previous 12 months. However, it was clear that vitamin A capsule distribution strategy needed to be modified. There were suggestions to combine the capsule distribution programme with other programmes such as mosquito net distribution or national Child Health Days. Recent data show that during the Child Health Days in June 2005, 82% of the targeted children received vitamin A capsules [24]. Figure 3 shows the trend in vitamin capsule distribution from 2003 to 2005. Some stakeholders believe that there is further need to formulate additional strategies for sustainable vitamin A capsule distribution and train staff involved in the implementation of the programme. For example, National Vitamin A days backed by vigorous information and education campaigns would help the parents to understand the need for their children to receive vitamin A supplements [23]. While the annual vitamin A capsule distribution campaigns together with the routine EPI should continue, more information should be given to mothers on the importance of this exercise. In addition, the staff involved should be well trained and motivated with sufficient supervision so that all the necessary details about the programme are recorded. DIETARY DIVERSIFICATION Dietary diversification leads to consumption of foods rich in pro-vitamin A. This is a sustainable and cost effective long-term strategy. However, recent studies showed that the efficiency of conversion of pro-vitamins in plant foods to retinol is variable. De Pee et al.[25] and Bulux et al.[26] suggested that there is little or no vitamin A nutritional benefit from increased consumption of dark green vegetables, highlighting the need to investigate this relationship further. While many Zimbabweans produce vegetables in their home gardens, there is insufficient documented information on consumption and preparation methods. In addition many people in the drier parts of the country do not have access to fresh vegetables throughout the year. Mandatory fortification of some staple foods, therefore, will help improve the nutritional status of consumers. FORTIFICATION OF FOOD WITH VITAMIN A Fortification of foods with vitamin A is technically feasible and can be a cost-effective method of providing adequate vitamin A to high risk groups [27]. According to current Zimbabwe laws [Food and Food Standards (Edible Fats and Oils) (Amendment Number 3) Regulations, 1990], vegetable oil is currently not required to be fortified with vitamin A. However, some food processing companies have voluntarily fortified vegetable oil with vitamin A. On the other hand, margarine is required to contain not less than 27 IU and not more than 33 IU of vitamin A [Food and Food Standards (Margarine) Regulations, 1973]. However, monitoring of these regulatory provisions is not very efficient as the central laboratories often do not have all the necessary materials (equipment and analytical reagents) and trained people to test for vitamin A in food. The laboratories, therefore, need to be well equipped to conduct these tests because fortification of vegetable oil and margarine are an efficient way of providing vitamin A to the consumers. Retention of vitamin A in vegetable oil has been reported to be as high as 83-100% after 6 months storage at 23oC [22]. Stability tests on vitamin A in maize meal and wheat flour have shown significant losses during storage and cooking [28]. For example, almost 32% of vitamin A added to maize meal was lost during 12 weeks storage at 45oC. Fortifying dry products such as cereal flours also requires a process of converting vitamin A to a water soluble compound and then drying it, which may increase fortification costs. Fortification of vegetable oil, therefore, seems to be the viable option in Zimbabwe and may result in sustained elimination of VAD in the country. Iron deficiency is one of the most widely prevalent micronutrient deficiencies in the world, affecting at least half of all pregnant women and young children in developing countries [3, 9]. Children under 24 months are especially at risk, resulting in stunting and reduced ability to resist common childhood illnesses [3]. In older children the ability to concentrate and perform well in school is lowered [29]. Anaemia is a serious risk to mothers with many women dying in childbirth because of severe anaemia. Iron deficiency anaemia in pregnant women reduces the oxygen supply to the foetus, causing intrauterine growth retardation and increased risk of premature delivery and reduced birth weight. Using results from the 1999 ZDHS, Mishra et al. [30] observed that supplementation of mothers with iron during pregnancy had a strong positive effect on child’s birth weight. When iron deficiency is compounded by other vitamin and mineral deficiencies, the economic impact can be significant, yet iron can be obtained from animal products such as red meat and in vegetables, grains and legumes. Chinyanga [31] measured the haemoglobin (Hb) levels in both goitrous and non-goitrous pregnant women in a survey done in Harare, Wedza and Nyanga. The study revealed that 11.4 % of the women in Harare had Hb levels less than 11g/dL, with 33 % in Wedza and 10.9 % in Nyanga. Folate levels of less than 2mg/mL in 7.8% of all the women assessed were also recorded. The Ministry of Health and Child Welfare also carried out an iron deficiency prevalence survey in 1997. Samples were collected in 4 provinces, namely, Mashonaland Central, Midlands, Matebeleland North and Matebeleland South. Haemoglobin and serum ferritin levels were measured in pre-school children, pregnant women, lactating mothers and adult males. It was observed that 33 % of pregnant women, 29.6 % of lactating women, 17.6 % of pre-school children and 16.5 % of adult males had Hb levels between 9 and 11g/dL. About 9 % of the population had depleted iron stores (serum ferritin <10µg/L), concluding that iron deficiency anaemia was of public health significance in Zimbabwe. It was suggested that future studies should examine the prevalence of parasitic infections and the HIV status of respondents in order to correct for their confounding effect. In a survey of 505 rural Zimbabweans in Matebeleland North province, iron overload was found almost exclusively among men who consumed traditional beer brewed in steel drums [32]. The study also reported high serum ferritin and a transferrin saturation of over 70%, raising concerns over possible high risk of liver disease. Maternal anaemia is a common cause of both maternal and neonatal mortality. The National Micronutrient Survey (1999) found that 31% of women of child-bearing age were anaemic, followed by children below the age of 6 years (27.4%) and children between 6 and 14 years (19.3%) [15]. Because of this, women in Zimbabwe are given iron supplements during pregnancy. Iron supplements distribution has been integrated with antenatal and postnatal health programme. Over 90% of pregnant women in Zimbabwe have at least one antenatal contact with the health services where they are expected to receive a four week supply of prophylactic iron sulphate and folate tablets. However, ZDHS (1999) recorded less than 6% of pregnant women had taken more than 90 iron tablets during their pregnancy [6]. Less than 5% of mothers in Mashonaland Central, Mashonaland East, Mashonaland West, Matebeleland North and Matebeleland South took 90 or more iron tablets during their pregnancy. In Harare, only 1% of mothers took 90 or more iron tablets during pregnancy. Zimbabwe Demographic and Health Survey (ZDHS) (2005/06) data also showed that in the five years preceding the survey, less than half (43%) of pregnant women received iron supplements. Women in urban areas were less likely to receive iron supplements than women living in rural areas (41 and 44%, respectively). Pregnant women in Harare are least likely to receive the supplements (29%). This is paradoxical considering the high number of pregnant women who have access to ante-natal care. Iron deficiency anaemia, therefore, continues to unnecessarily hamper national productivity. OTHER MICRONUTRIENT DEFICIENCIES Seasonal niacin deficiency and cases of pellagra have been reported in Zimbabwe, increasing during severe drought. Niacin deficiency is associated with a maize based diet. Surveillance reports from Mashonaland Central indicated high incidence of pellagra in 1995 [33]. Data from the NHIS shows that pellagra cases have been on the increase since 2000, with 5538 cases reported in 2005 compared to 3832 in 2000. Vitamin B12 levels were reportedly low in some pregnant women in Zimbabwe [31]. There is, therefore, need to address these micronutrients in the broader strategy to reduce VMD. STAPLE FOOD FORTIFICATION IN ZIMBABWE The objective of national micronutrient programmes is to ensure that needed micronutrients are available and consumed in adequate quantities by vulnerable groups. The micronutrient deficiencies described above highlight the inadequacy of the diet to provide adequate amounts of the micronutrients. Household food insecurity forces people to consume the little food that is available with very little scope for diversification. From the consumption studies previously done in Zimbabwe, it is apparent that mandatory fortification of staple foods such as maize meal, wheat flour, sugar, cooking oil and salt, which are commonly consumed by vulnerable groups in the population may help to reduce and eventually eliminate most of the micronutrient deficiencies in Zimbabwe [34, 35, 36]. Fortification of salt with iodine has been a major success with more than 95% of the population now using iodised salt. The fortification of maize meal or flour with iron and folate is feasible, inexpensive, safe and likely to be beneficial, while the fortification of vegetable oil with vitamin A has been done elsewhere with great success [37]. Vitamin A fortification of sugar is currently being done in Zambia and Nigeria. However, experience with sugar fortification in Zambia shows that sugar processors are likely to pass on the cost of fortification to the consumer and that imported sugar has to meet the fortification requirement. The size of sugar granules also affects the efficiency of fortification, hence the need to assess feasibility for specific countries. THE WAY FORWARD According to WHO criteria for elimination of IDD, Zimbabwe achieved Universal Salt Iodisation (USI), with repeated surveys since 1995 indicating that more than 90% of the households in Zimbabwe use iodised salt. Salt monitoring and surveillance should be done on a continuous basis. The country should also pursue mandatory fortification of edible oils. Available food consumption data show that more than 60% of the population consume vegetable oils almost every day. In addition, mandatory fortification of wheat flour with iron and folic acid is also feasible with the bulk of the flour being produced by five big companies. However, many small millers have emerged as key suppliers of maize meal and flour and have to be considered in any strategy for food fortification. Flour and maize meal can also be fortified with B-group vitamins. The Food and Nutrition Surveillance is a good tool to monitor the progress towards eliminating VMD. It is recommended, however, that a more representative sampling frame be used so that a better estimate of the micronutrient status in the country is readily available. The IDD Sentinel surveillance should be integrated into the Food and Nutrition Surveillance in order to maximise the use of resources. The National Micronutrient Surveys should also be held timely to allow for effective intervention. CONCLUSION Although the country has recorded significant progress in reducing malnutrition, significant setbacks have been observed in the last 5 years, especially due to drought induced food shortages. This has also impacted the micronutrient nutrition status of the population. However, the control of IDD in Zimbabwe seems to have been successful. The national total goitre rates have been decreasing since 1988 and up to 95% of households in Zimbabwe used iodised salt and the median urinary iodine levels are about 220 μg/L. On the other hand the main strategy against vitamin A deficiency has been vitamin A capsule distribution during routine visits to clinics for growth monitoring and immunisation. A national coverage of 22.3% by March 2005 suggests that the programme may not be achieving its intended goal. Vitamin A capsule distribution during Child Health days, however, seems to be more effective as up to 90% of the targeted children are reached. The impact of other micronutrients such as vitamin B group and zinc have not been thoroughly investigated and there is need for the country to strengthen the micronutrient intervention programmes in order to achieve some of the Millennium Development Goals [38]. ACKNOWLEDGEMENT This review was made possible with funding from Helen Keller International under CIDA purchase order 7036919. The views in the paper do not reflect opinions of either HKI or CIDA. REFERENCES
© Copyright 2009 -Rural Outreach Program The following images related to this document are available:Photo images[nd09003f1.jpg] [nd09003f3.jpg] [nd09003f2.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}