 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Dermatology, Venereology and Leprology, Vol. 75, No. 2, March-April, 2009, pp. 214-216 Resident's Page Pap smear Mehta Vandana, Vasanth Vani, Balachandran C Department of Skin and STD, Kasturba Medical College, Manipal, Karnataka Code Number: dv09069 Introduction Cervical cancer is predominantly sexually transmitted and the association between certain oncogenic (high risk) strains of human papillomavirus (HPV) and cervical cancer is well documented. [1] It has been shown worldwide that screening for precursors of cervical cancer by means of Papanicoloau (Pap) smears substantially reduces the incidence of invasive cancer.[2]Definition A Pap smear, also known as Papanicoloau smear, is a microscopic examination of cells scraped from the cervix and is used to detect cancerous or pre-cancerous conditions of the cervix or other medical conditions. It was named after Dr. George N. Papanicoloau, who first described it in 1928 and since its introduction, the Pap smear has helped reduce cervical cancer incidence and mortality rates by 75%. The Pap smear is a screening tool that looks for changes in the transformation zone of the cervix, which most often are caused by HPV.Method of Sample Collection The cervix is composed of columnar epithelium, which lines the endocervical canal, and squamous epithelium, which covers the exocervix. The point at which they meet is called the squamocolumnar junction. Metaplasia advances from the original squamocolumnar junction inwards toward the external os and over the columnar villi, which establishes an area called the transformation zone. It is this area that the sample is taken from for the Pap smear. Screening with conventional Pap testing should occur every year. If liquid-based cytology (LBC) is being used, screening can be extended to every 2 years. Screening should begin at the age of 21 or within 3 years of the onset of sexual activity and it can stop at the age of 70 years if there has been no abnormal Pap test result in the past 10 years. [3] A Pap test should be performed during the second half of the menstrual cycle (Day 14). Sample collection usually begins with appropriate instruction to the patient. Patients must abstain from sexual intercourse and avoid using any vaginal medication or contraceptives 48 h before sample collection. The patient is placed in lithotomy position and the cervix is visualized by means of a speculum. The smaller end of the Ayre′s spatula is introduced through the external os and the squamocolumnar junction is scraped by rotating the spatula to 360°. The scraping is then evenly spread onto a glass slide, which is immediately fixed using 95% ethyl alcohol and ether to avoid air drying artifacts. [4] What is an Adequate Smear? An adequate smear is the one with the following features:
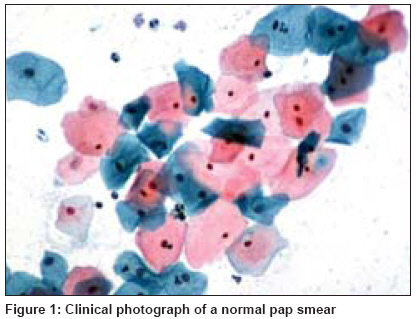
Interpretation of a Normal PAP Smear The following three types of cells are seen in a normal Pap smear:
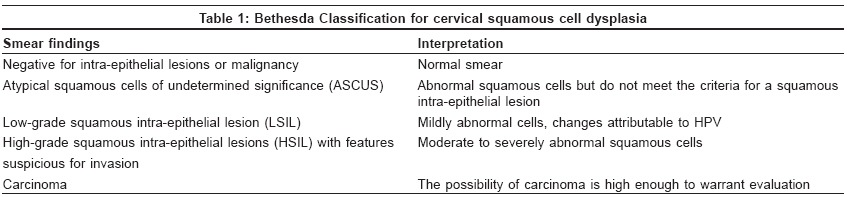
PAP Smear Reporting The Pap smear reporting classification has evolved and been refined over time. The current reporting system is the Bethesda system, which was introduced in 1988 [6] and later updated again in 1999 [Table - 1]. [7] Patients with abnormal Pap smear who do not have a gross cervical lesion are usually evaluated by colposcopy- and colposcopy-directed biopsy. Colposcopy can detect low- and high-grade dysplasia but does not detect microinvasive disease. Colposcopy is the study of cervical morphology using stereoscopic binocular magnification provided by the colposcope. This instrument provides a 3-dimensional image of the examined tissue surfaces and its use is now routinely recommended for the evaluation of abnormal Pap smears. In screening programs aimed at detecting and eliminating cervical cancer and pre-cancer, colposcopy plays an important adjunctive role with cytology and histology. If no abnormalities are found or if the entire squamocolumnar junction cannot be visualized, a cervical cone biopsy or HPV DNA test is performed. Limitations of PAP Smear
Newer Techniques A conventional Pap smear has a sensitivity ranging from 47 to 62% and a specificity of 60-90%. In order to minimize the number of false-negative results, LBC is now the preferred method of sample collection where a cervical brush is used to collect the specimen, which provides almost twice as many epithelial cells. The samples are collected directly in a preservative solution and slides are prepared meticulously avoiding any uneven manual smearing and thus reducing human error while interpretation. LBC has got a higher sensitivity and specificity than Pap smear as the cellular structure is better preserved because the cells are fixed immediately. [8] Another way to improvise the Pap smear diagnosis is by using stains to detect the HPV antigens. [9]Conclusion All sexually active women must have a Pap smear examination annually to detect cervical cancer. If the smear is abnormal, it is repeated at 3-6 monthly intervals. Three abnormal results in a row is a definite indicator for further evaluation.References
Copyright 2009 - Indian Journal of Dermatology, Venereology and Leprology The following images related to this document are available:Photo images[dv09069t1.jpg] [dv09069f1.jpg] |
| |||||||||

{kind=link}
{kind=link}