 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Surgery, Vol. 66, No. 2, Mar-Apr, 2004, pp. 70-74 Laparoscopic surgery of inguinal hernia in children - experience with 110 repairs Sanjay Oak, Sandesh Parelkar, Prakash Agarwal, Manjusha Sailukar, Parshottam Gera, Rahul Pathak, Naveen Viswanath Department of Paediatric Surgery, T. N. M. C. and B. Y. L. Nair Hospital,
Mumbai - 400008, India. Paper Received: December 2003. Paper Accepted: February 2004. Source of Support: Nil. Code Number: is04017 ABSTRACT Background: Laparoscopic inguinal herniorraphy has
been in practice in adults since its initial description by Ger in 1921. However
there is no standardized technique for children until now. We present a series
110 repairs of hernias in infants and children treated laparoscopically. The
aim of this study is to document authors' experience with laparoscopy in inguinal
hernia in girls and boys.
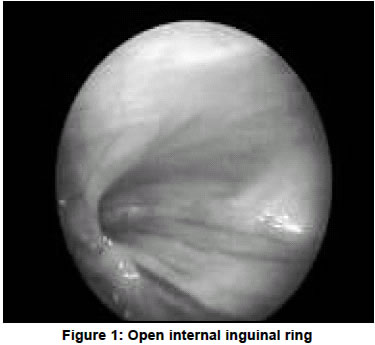
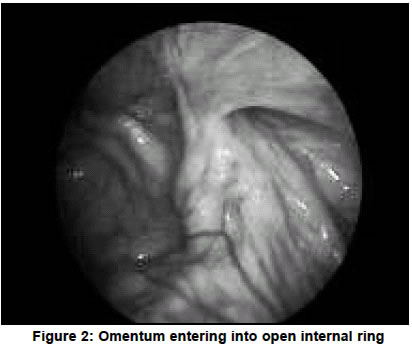
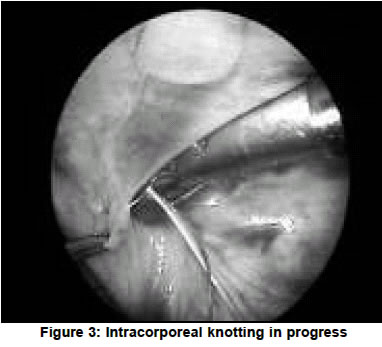
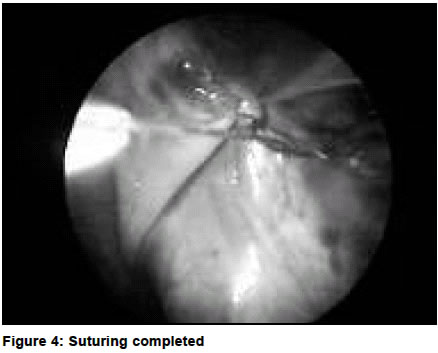
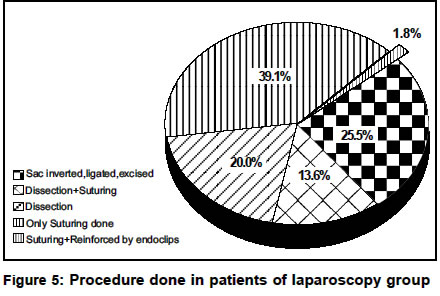
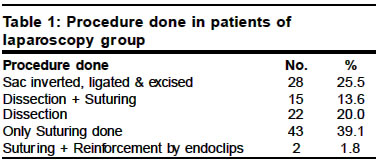
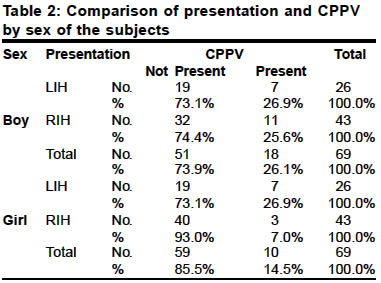
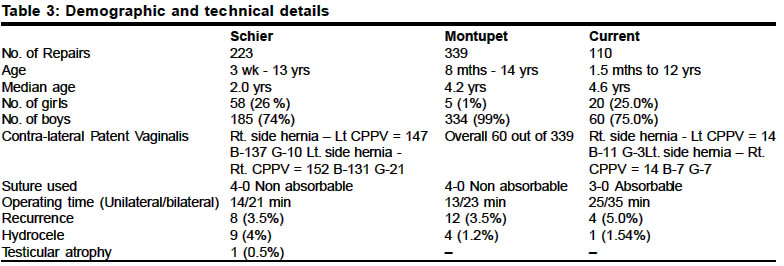
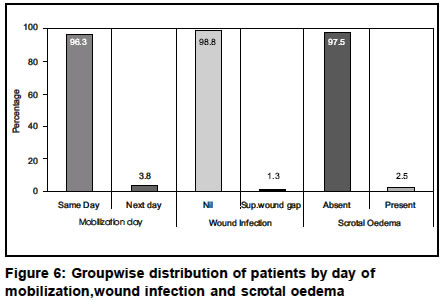
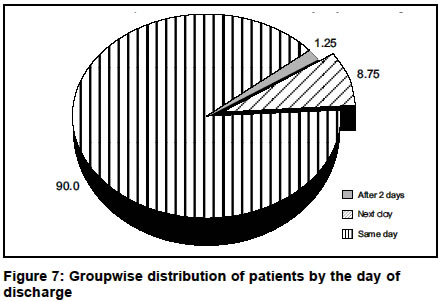
Key Words Paediatric inguinal hernia in children, Laparoscopic repair of inguinal hernia in children, Laparoscopy. How to cite this article: Oak S, Parelkar S, Agarwal P, Sailukar M, Gera P, Pathak R, Viswanath N. Laparoscopic surgery of inguinal hernia in children - experience with 110 repairs. Indian J Surg 2004;66:70-4. INTRODUCTION Laparoscopic inguinal herniorraphy has been in practice in adults since its initial description by Ger in 1921.1 Inguinal hernia in children most often presents as a simple opening at the internal inguinal ring and a patent processus vaginalis (PPV). They require surgical treatment for definitive occlusion of orifice. A PPV at birth is a common event occurring in approximately 25% of boys.2 Protrusion of PPV presents as a potential hernia and approximately 10% of these develop a clinical hernia. The issue of bilaterality is also of significance in paediatric age group. The detection and management of occult contralateral hernia in children who present with a clinically evident unilateral hernia has also evoked controversy. Historically, Duckett first commented on the frequency of the appearance of contralateral hernia.3 And Rothenberg and Barnett proposed routine bilateral exploration.4 Sparkman reviewed this issue and found that routine contralateral exploration reveals a PPV in 50 to 60% of cases.5 However this contralateral processus vaginalis would progress to a clinically apparent hernia in only 8 to 15% of patients.6 Several methods have been attempted to evaluate contralateral groin and a laparoscopic repair of the side with which patient presents, gives the patient the best possible opportunity to inspect and repair the contralateral PPV. This study was undertaken to evaluate feasibility, safety and efficacy of the repair of inguinal hernia in children laparoscopically. MATERIAL AND METHODS This study was conducted at a university teaching general hospital between Dec. 2000 and Dec. 2002. Appropriate informed consent was obtained from all patients. Laparoscopic inguinal herniotomies were performed in 80 children (60 boys and 20 girls). Because of bilaterality, 110 defects were closed. The youngest patient was 1.5 months old and eldest was 12 years of age. The median age of patients was 4.6 years. 43 hernias were on right side (53.7%), 26 were on the left side (32.5%) and 11 hernias were bilateral (13.7%). A 5 mm laparoscope was introduced through umbilical port. Two 3 mm or 5 mm instruments (one needle holder and Maryland forceps) were inserted through the pararectal lateral abdominal wall. The abdominal cavity was inspected. Open internal inguinal ring more than 2 mm in size was selected for elective repair (Figures 1 and 2). Intracorporeal suturing was done with 3-0® Vicryl by either a purse-string or a Z type of suture (Figures 3 and 4). The needle was inserted directly through abdominal wall and removed along with trocars. The umbilical fascia was closed with absorbable suture. The skin was closed with absorbable subcuticular suture. RESULTS In the 2 years of study, 110 defects were repaired in 80 patients. There were 60 boys and 20 girls. The median age of patient was 4.6 years. The youngest was 1.5 months female and eldest was 12 years of male. Clinical presentation in outdoor clinics revealed that 43 cases were right sided, 26 left sided and 11 children presented with bilateral hernias. However, laparoscopy revealed that in 27 patients there was a significantly open contralateral internal inguinal ring and a PPV, which necessitated repair. In 28 defects in female hernias an endoloop was passed, the sac was ligated and the redundant sac was excised. In 22 defects, the sac was only dissected and the raw area created by this dissection was left alone. In 15 defects, intracorporeal suturing was done after dissection of sac, whereas in 43 defects only intracorporeal suturing was done without dissection (Figure 5 and Table 1). In 2 patients an intracorporeal suture was also reinforced by the application of small size endoclips to approximate medial and lateral pillars of internal inguinal ring. The operating time showed a decreasing trend as the experience of the team is increased. A unilateral repair required 25 minutes and a bilateral repair 35 minutes. Preoperative diagnosis of a right sided hernia was found to be incorrect in 2 patients (2.5%) on laparoscopy because the ring was completely closed. The asymptomatic contralateral internal inguinal ring was routinely evaluated for a PPV. If the hernia was present on the right side, a left side patent PPV was found in 25.5% (11 out of 43) of the boys and 6.9% (3 out of 43) of girls. If the hernia was on left side, a contralateral PPV was found in 26.9% (7 out of 26) of boys and 26.9% (7 out of 26) of girls (Table 2). Openings smaller than 2 mm (the size of the needle holder shaft) were unlikely to cause hernia and were left open. The recurrence was seen in 4 cases (5%). This recurrence was seen in the early phase of study where the surgical team was in the initial learning curve of technique and the selection of cases for laparoscopic repair was not standardized. Although this recurrence rate is comparable to other current series of laparoscopic pediatric hernia repair the rate for open herniotomies in different series is between 0-1%.10 The rates of recurrence will fall as the experience in laparoscopic pediatric hernia repair increases and standardization of the procedure takes place, therefore we recommend that such surgery be carried out only by those who have undergone advanced training in this field. The follow up period ranged from 2 months to 2 years. No direct inguinal hernia was seen. Postoperative hydrocele occurred in one boy which settled by conservative management. Testicular atrophy was not noticed (Table 3). Except for babies of less than 3 months of age, all other children left the hospital on the day of operation (Figures 6 and 7). DISCUSSION Inguinal hernia repair is one of the most common operations performed in children. As shown by the results in this series, this operation has a high success rate and a low complication rate. However its treatment is still controversial because of three main aspects; the exploration of the asymptomatic contralateral side, the incidence of complications related to the possible damage of the vas deferens or the spermatic vessels, and the complications related to the surgical technique; such as recurrence, nerve entrapment or a nerve section (Ilioinguinal, iliohypogastric branches).7 Given the possibility of the development of contralateral hernia in a relatively high percentage of patients soon after unilateral repair, some surgeons prefer to perform bilateral approaches.8,9 Several investigators have acknowledged that routine bilateral exploration would disclose a contralateral sac in about 50% to 90% of cases but contend that only a small percentage of these sacs (5.6% to 16%) would evolve into clinical hernias.10,11 Therefore it is opined that routine exploration based on the likelihood of a patent processus vaginalis (PPV) according to age, gender or side of hernia would lead to unnecessary procedures. Laparoscopy offers a quick, safe and cost-effective method to detect a patent PV.11 Laparoscopy either through an umbilical port or more commonly through the opened processus vaginalis of the traditionally opened side with the use of a 700 or 300 scope has been used extensively by many authors.12-20 Positive results were visible patency of processus vaginalis or bubbles or fluid and/or gas expressed from the processus by palpation.13 Laparoscopy; in a number of patients shows open internal rings. These patients may not even have a history of "hernia". The internal ring itself has several variations. The ring may appear completely closed and flat or it may be very widely open.21 Clefts and veils of peritoneum sometimes make determining the exact anatomy difficult. Characterization of the anatomical variability of the internal ring is essential for determining the patency of the processus vaginalis at laparoscopy in children with a known inguinal hernia. Rings more than 2 mm in size merit closure by approximation of medial and lateral pillars. Our technique includes 5mm of O0 laparoscope inserted through the umbilical port and two pararectal 3 mm ports through which hand instruments are inserted. Initial attempts of circumferentially incising and dissecting the sac from cord structures were subsequently abandoned. As there is no difference in the laparoscopic access for unilateral and bilateral hernias; bilaterality presents no problem for laparoscopic technique. An obviously open ring is closed; a questionably open ring is closed as well. In girls with inguinal hernias containing ovaries, laparoscopy permits inspection of internal genitalia and easy withdrawal of prolapsed ovaries back into the peritoneal cavity.1n open surgery, this is more difficult and traumatic. The operating time is comparable with that for a conventional open procedure. With practice; the median operating time decreased for both unilateral as well as for bilateral repairs. In two patients; endoclips were used to reinforce the suture approximation of internal ring. The recurrence rate in our series appears higher than that generally accepted for open repair. This is at least in part caused by early learning curve and improper selection of a patient. Babies less than three months of age and having a large sized hernia and/or a very wide open internal ring should not be selected as candidates for a laparoscopic repair in the initial learning phase of the technique. If the recurrence should arise after the laparoscopic operation; the surgeon and parents could have a choice between a conventional approach at the second time or a re-laparoscopy. Out of four recurrences in our series, three cases were managed with open herniotomies and one hydrocele resolved spontaneously. An additional benefit of laparoscopic repair is that in laparoscopic herniotomy, there is no dissection of cord structures. Therefore, the risks of superior displacement of the testicle culminating into acquired undescent; testicular atrophy; injury to the vas are practically never seen. The most common difficulties after conventional hernia surgery such as local edema, haematoma and wound infection are absent after laparoscopic technique. Among the possible disadvantages of this type of hernia repair are the requirement for general endotracheal anesthesia for laparoscopy and the presence of a suture on the pelvic wall. Postoperative development of hydrocele in the distal sac has been well reported in 0.6%- 1% of cases by various authors.22 Most of these resolve over a period of 3-6 months. Experimental study aimed at chemical obliteration of distal processus vaginalis with 6% .iodine solution has been carried out in rat and the results of this study are promising and beneficial for successful laparoscopic indirect inguinal hernia repair in children. CONCLUSION The early results of this series thus indicate that laparoscopy is cost-effective (detailing the costs of supplies, operating time, length of study, early return to unrestricted activity, reduction in period of absence from job for the parents), cosmetically superior, safe and feasible for bilateral repair in the same sitting. REFERENCES
© 2004 Indian Journal of Surgery. The following images related to this document are available:Photo images[is04017f3.jpg] [is04017f1.jpg] [is04017f4.jpg] [is04017f5.jpg] [is04017f2.jpg] [is04017t2.jpg] [is04017f6.jpg] [is04017t1.jpg] [is04017t3.jpg] [is04017f7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}