 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 1, 2002 pp. 52-53 Necrotising Histiocytic Lymphadenitis Pandey M, Abraham EK, Somanathan T, Sebastian P Department of Surgical Oncology and Pathology, Regional Cancer Centre, Thiruvananthapuram
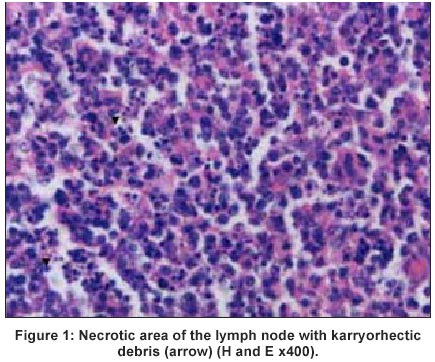
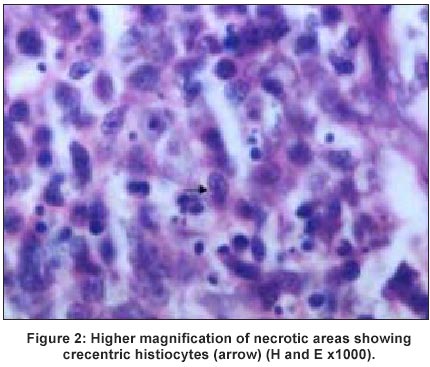
- 695 011, India Code Number: jp02016 A 13-year-old male presented to outpatient clinic with swelling right side of the neck of two months duration. There was no history of fever, malaise or weight loss. Haematological and biochemical parameters were normal. General blood picture showed hypochromic red cells, normal white cell count with occasional atypical lymphocyte and adequate platelets. Examination revealed multiple 1x1 cm soft to firm lymph nodes in right supraclavicular, lower jugalodigestric chain and in both axilla. Left neck, other areas of right neck and inguinal areas were normal. Abdominal and per rectal examination did not reveal any abnormality. A clinical diagnosis of Hodgkin's disease was made and an excision biopsy of right supraclavicular node was performed. Microscopic examination of lymph node showed retained architecture with hyperplastic follicles having prominent germinal centres. There was marked paracortical expansion with sheets of histiocytes showing karyorrhexis, surrounding mature lymphocytes were admixed with immunoblasts. A diagnosis of necrotising histiocytic lymphadenitis was made (Figure 1 and 2). No treatment was offered to the patient in light of the diagnosis and patient was lost to follow-up.
Discussion Kikuchi's disease (KD) is seen predominantly among women in their third and fourth decade of life.1 The disease is more common among Asians in general and Orientals in particular. It is relatively rare in south East Asia. The disease primarily affects cervical lymph nodes and has a self limiting clinical course, however, a low recurrence rate of 3.3% is reported.2 Extranodal involvement specially of the skin has been reported by several authors.2,3,4 The disease has unknown aetiology. Infection is often considered as an inciting agent. It is hypothesised that lymphokine production in an immunocompromised host may result in histiocytic proliferation. Association with Epstein-Barr virus, human herpes virus 6 and 8, Parvovirus B-19, Human T-cell lymphocytic virus, Human immunodeficiency virus, Toxoplasma gondii and Yersinia enterocolitica has been demonstrated.5,6 Huh et al7 investigated viral aetiology for KD. They performed a polymerase chain reaction (PCR) in 12 freshly frozen lymph nodes from patients with KD and found no amplification for EBV, Herpes Simplex Virus (HSV) type I, HSV type II, and cytomegalo virus (CMV), excluding the role of these viruses in pathogenesis of KD.7 Raised levels of IL6 and IFN-r are demonstrated in all the patients during acute phase, which returned to normal during convulsant phase. The histological findings of KD are distinctive. Patchy areas of necrosis without a polymorphonuclear leukocyte infiltration is characteristic finding. The necrotic areas show prominent karyorrhetic debris, immunoblasts, histiocytes and plasmacytoid T-cells/ monocytes. The histiocytes have a C-shaped nuclei and some contain cellular debris.8 At times there is little or no evidence of necrosis, but karyorrhetic debris will be present. The lymph node shows patchy infiltrate consisting of immunoblasts, plasmocytoid monocytes and histiocytes with a paucity of plasma cells. Immunohistochemistry shows a positive immuno- staining by antibodies Mac 387, KP1 (CD68) and KiMIP. In addition a variable number of T-cells immunostained by antibody MT1 (CD43) or UCHL1 (CD45 RO) are also seen.2 CD8+ T-cells identified by antibody C8/144 were observed in all lesions, however, the expression varied from few cells to abundant. DNA analysis by flowcytometery in limited number of cases revealed a diploid DNA. The mechanism of cell death has not been extensively studied and no definitive aetiology has been identified. Presence of nuclear DNA fragmentations in lymphocytes and histiocytes present around the area of necrosis suggest a possible role of apoptosis in cell death. Since the morphological features encountered in a lymph node are distinctive, it enables the pathologists to diagnose KD with confidence. Nonetheless, difficulty is encountered at times in differentiating it from certain malignant and benign disorders. It is not infrequently diagnosed as non-Hodgkin's lymphoma (NHL) or Hodgkin's disease (HD). High grade NHL with necrosis and karyorrhesis may be differentiated from KD by the lack of the larger cells with twisted nuclei seen in Kikuchi and additional evidence of lymphoma in the other parts of the lymph node. In case of the KD with focal lesions consisting of immunoblasts and histiocytes with no evidence of necrosis, it is very difficult to distinguish from lymphoma.9 The presence of definite Read Sternberg cells helps in distinguishing HD from KD. Necrosis associated with HD usually contains polymorphonuclear leukocytes, which are absent in KD.9 Of the benign disorders the most important is systemic lupus erythematosis (SLE). Since some patients of KD have later developed SLE and since the necrotic lesion in the lymph node are similar it has been suggested that necrotising histiocytic lymphadenitis may be a `forme firste' of SLE.8 Presence of numerous plasma cells and/or granulocytes, haematoxylin bodies and coagulative type of necrosis without karyorrhetic debris suggest SLE, rather than KD.10 Other entities included in the differential diagnosis are Cat Scratch disease (CSD), Infectious Mononucleosis (IMN), Toxoplasmosis and Kawasaki's Disease. The presence of microabcess distinguishes KD from CSD. The diagnosis of IMN is made on the basis of characteristic clinical, haematological and serological findings. Toxoplasmosis on the other hand, is characterised by a triad of histological findings: follicular hyperplasia, cluster of epithelioid histiocytes and prominent parafollicular monocytoid B cells. Positive serology for toxoplasma confirms the diagnosis. Kawasaki's Disease or mucocutaneous lymph node syndrome is an acute febrile illness in children associated with nonsuppurative cervical lymph adenopathy. Lymph node biopsy shows foci of necrosis with adjacent intracapillary fibrin thrombi. The clinical settings and the characteristic histological findings in the lymph node helps in differentiation.10 In patients presenting with pyrexia of unknown origin with cervical lymphadenopathy lymphoma and tuberculosis are two common clinical diagnoses in our country. Differentiating these from the other benign lesions poses difficulty, as most of the IHC markers are not available in most of the laboratories. Although there are not many cases reported earlier, we presume this to be a result of ignorance rather than disease rarity. It is important for pathologist and clinicians to be aware and keep this possibility in mind specially when dealing with young female patient with fever and cervical lymphadenopathy.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02016f2.jpg] [jp02016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}