 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
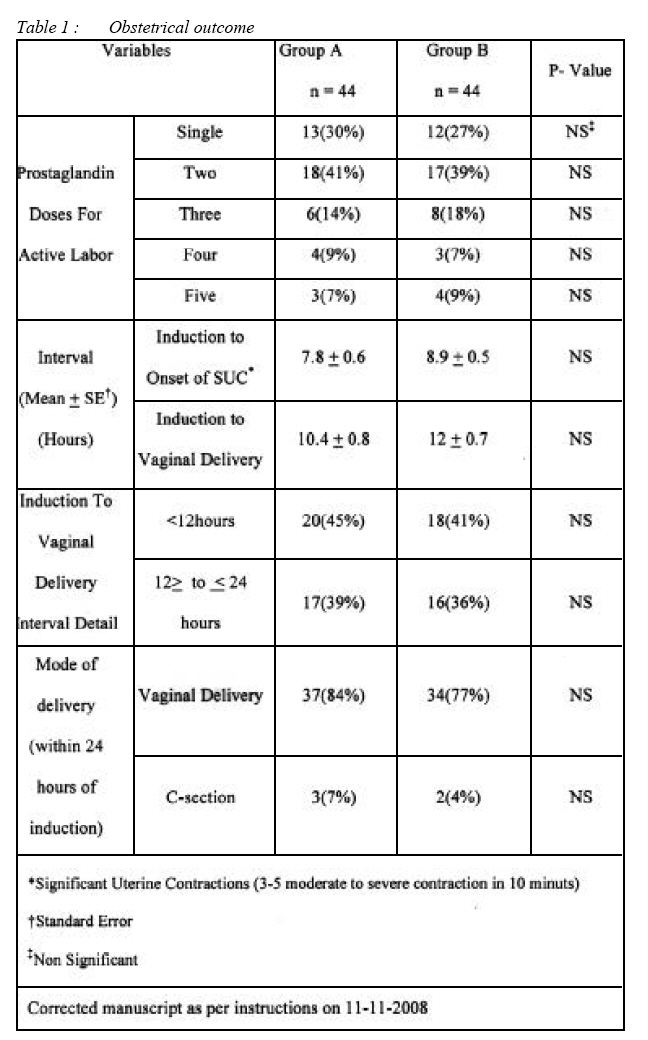
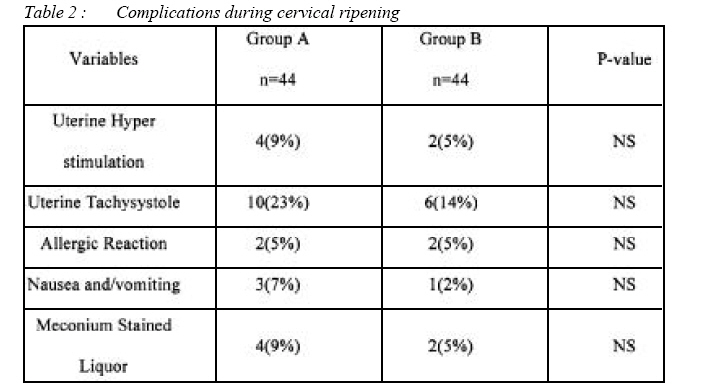
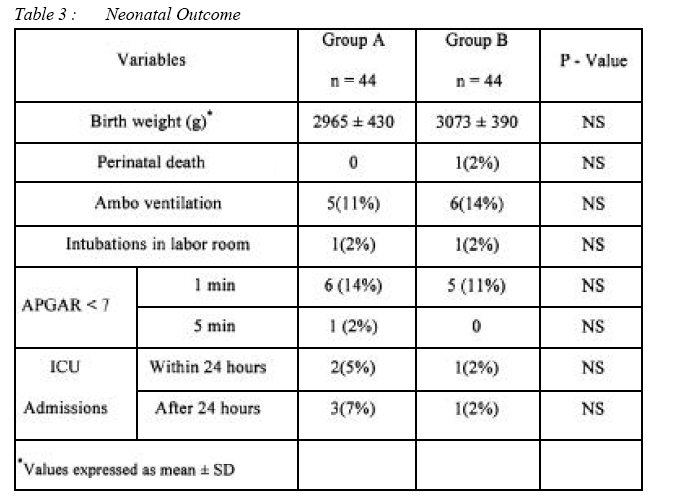
ORIGINAL ARTICLE Labor induction with randomized comparison of oral and intravaginal misoprostol in post date multigravida women Aqueela Ayaz, *Shazia Saeed, **Mian Usman Farooq, ***Iftikhar Ahmad, ****Muhammad Luqman Ali Bahoo, *****Muhammad Saeed Specialist Ob/Gyne, Hera General Hospital, Makkah, Kingdom of Saudi Arabia Submitted-20-02-2007, Accepted-03-12-08 Code Number: mj09005 The efficacy and safety of oral versus vaginal misoprostol for elective induction of labor in post date multigravida with an unfavorable cervix was compared over a period of a year in the Bahawal Victoria Hospital, Bahawalpur, Pakistan. Eightyeight ultigravida post date women were divided into two groups and given 50 mcg misoprostol orally and 50 mcg intravaginally, respectively. The induction onset of significant uterine contractions and delivery intervals were lower in the first group (7.8 h vs. 8.9 h) when compared to (10.4 h vs. 12 h). The first group had a higher rate of Caesarean section (7% vs. 4%; p>0.05), uterine hyperstimulation (9% vs. 5%; p>0.05), uterine tachysystole (23% vs. 14%; p>0.05) and neonatal admissions to intensive care unit (12% vs. 4%; p>0.05) when compared to second group. 50 mcg oral misoprostol has the potential to induce labor as safely and effectively as the intravaginal route. Key words : Misoprostal, induction, labor Introduction Lingering pregnancy is one of the most common indications of labor induction even though it has been carried out also for other indications of maternal and fetal origin and it has been done for approximately one in six pregnancies exceeding 24 weeks’ gestation in the United States (1). Recent studies have suggested that by continuing pregnancy beyond 41 weeks, there is a statistically significant higher perinatal morbidity and mortality as well as an increased risk to the mother (2, 3). Attempted induction with an unripe cervix is exigent and seldom results in success (4). Although many methods of preinduction cervical ripening have been anticipated but prostaglandins are the up to date agents of choice (5, 6). A lot of evidences have highlighted the importance of prostaglandins for initiation and normal progress of labor (7) as well as to induce cervical ripening and stimulate uterine contractions at a variety of doses and routes of administration i.e. orally or vaginally (8, 9). Misoprostol have been compared satisfactorily with the presently agreed agent dinoprostone in cost and storage requirements. The most advantageous dosing regimen, timing, and route of administration lingered the focus of enduring research (10–12). Misoprostol is reasonably priced synthetic prostaglandin E1 analogue (13), and its oral administration has obvious appeal because it offers ease and higher patient satisfactoriness and promises outpatient administration if proved safe and effective for cervical ripening and labor induction but it has been studied less comprehensively. This study was a comparative analysis of the effectiveness and safety of oral misoprostol and intravaginal misoprostol for the use in the process of cervical ripening and inducing labor in multigravida postdate pregnancies with a live fetus. Material & Methods This study was conducted from December 1, 2004 till November 30, 2005. 88 women were selected for the study where 44 were randomised in the oral group (group A) and the remaining in the intravaginal group B. All of the women were recruited at Bahawal Victoria Hospital, Bahawalpur, Pakistan, a 1300 bedded tertiary referral center with an average annual delivery rate of 2500. The Hospital Research Committee approved the study and all participants gave their written informed consent after they had been made aware of the purpose of the study. Inclusion criteria were those whose age were between 26-40 years, multigravida, accurate dating of gestation, singleton viable pregnancy, gestational age 40 - 42weeks, cephalic presentation, unfavorable cervical status defined as a Bishop score (BS) of <6, intact membranes, patient’s height more than 150cm. Exclusion criteria were patients with known contraindications to receiving prostaglandins, placenta previa, previous uterine surgery and any antenatal complications (medical/obstetrical). The detailed history with general physical examination included vital signs and abdominal examination. A fetal cardiotocographic (CTG) trace to confirm fetal well being was performed. Digital examination was done to confirm the BS. Baseline investigations included complete blood & urine examination, blood grouping and Rh factor were sent. Gestational age was estimated by ultrasound biometry via Crown rump length (CRL) measurements in the first trimester of pregnancy in cases where there was more than 3 days difference from that obtained from the last menstrual period (LMP) (14). Uterine tachysystole was defined as >5 contractions of moderate to severe intensity per 10 minutes, uterine hypertonus as when one contraction lasted more than 2 minutes and hyperstimulation syndrome as the presence of non-reassuring FHR tracing combined with either tachysystole or hypertonus (15). The patients were divided into group A and group B by randomization for induction with oral and vaginal misoprostol, respectively. The randomization was done by opening sequentially numbered opaque envelops containing cards stating the drug for induction. Bishop’s score was performed prior to administration of either preparation, if it was less than six; the patient was planned for induction of labor. Misoprostol of 50 mcg tablet was given orally for induction in group A, and in group B induction was done by placing same dose high in posterior fornix digitally, tablets were repeated after every four hours to a maximum of six doses if there was no uterine activity or if the uterine contractions were less than two mild contractions in ten minutes with the patient being comfortable. Fetal CTG was done to confirm fetal well being before each close. When uterine activity suggested the onset of labor, vaginal assessment was performed and the women will be sent to the labor ward. During all the proceeding maternal vitals were monitored at 4 hours interval. The time of dose introduction, beginning of significant uterine contractions (significant uterine contractions mean 3-5 contractions of moderate to severe intensity in 10 minutes) and delivery was noted. Adequate analgesia (pethidine) was given. Continuous fetal & maternal monitoring and progress of labor was recorded on partogram. Failed induction of labor was defined as vaginal delivery not achieved within 24 hours of initiating induction of labor (16). The indications for Cesarean section (CS) were failed induction, maternal request after 24 hours of induction, uncontrolled hyper stimulation and fetal distress. The complications faced during induction procedure were recorded carefully and managed accordingly. Pediatrician was called to examine and resuscitate the baby at the time of delivery. Further management of neonates was done accordingly. The primary outcome measures were time from induction to onset of significant uterine contractions and induction to delivery. The secondary outcomes were the CS rate, the incidence of uterine tachysystole, uterine hyperstimulation and fetal/neonatal complications. Data was analyzed on SPSS and subjected to descriptive analysis. Z-Test: Two samples for mean were applied to numerical data (interval of induction to significant uterine contractions and delivery) while remaining categorical data was analyzed with Chi-squared test. P-value <0.05 was considered as significant. Results Mean age in group A was 34.3 as compared to 35.9years in group B, while mean + standard deviation (SD) of gravidity was 3.6+1.6 in group A and 3.2+1.4 in group B respectively. On the other hand, mean + SD of parity in group A was 2.9+1.1 while group B had 2.4+0.9. In group A 13(30%) subjects had active labor after insertion of single dose of misoprostol as compared to 12(27%) in group B. The mean + standard error (SE) of induction to onset of significant uterine contractions interval was 7.8 + 0.6 hours in group A, while 8.9 + 0.5 hours in Group B (p>0.05). Similarly the mean induction to delivery interval was 10.4 + 0.8 hours in group A while 12 + 0.7 hours in group B (p>0.05). Failed induction was little bit less frequent in group A than group B (16% vs. 23%; p>0.05). (Table 1) There were more subjects with uterine hyperstimulation and tachysystole in group A than group B i.e. (14% vs. 5%; p>0.05) and (23% vs. 14%; p>0.05) respectively but statistically not significant. Cesarean sections were performed in all subjects with uterine hyperstimulation syndrome in both groups. Meconium stained liquor was also found in four subjects in group A. (Table 2) There were more neonatal admissions to intensive care unit in group A (12% vs. 5%; p>0.05). Perinatal death was noted in group B due to meconium aspiration syndrome. (Table 3) Discussion Interest in oral misoprostol for cervical ripening and labor induction is growing day by day(17-21).The present study was the one that compared oral misoprostol with intravaginal in such wellhomogenized groups. All of the women were multigravida with intact membranes and at more than forty weeks’ gestation with no antenatal complications. Our rationale was to identify effectiveness and safety of oral misoprostol regimen with intravaginal regimen. We found that giving 50 mcg of misoprostol every 4 hours was as effective and safe as vaginal administration of 50-mcg doses every 4 hours, with no significant differences in maternal or neonatal outcomes. Although not statistically significant, in group A we found shorter mean intervals from start of induction to delivery and a higher propensity for vaginal delivery within 24 hours. In previous studies, 50 mcg of oral misoprostol given every 4 hours was associated with longer intervals to delivery compared with vaginal misoprostol (13, 20). In one Egyptian research, 100 mcg of oral misoprostol was administered to 20 subjects, then doubled the dose after 3 hours if there was inadequate clinical response. They compared that regimen with repeated doses of 100 mcg of vaginal misoprostol and found greater efficacy but more fetal heart rate and uterine contraction abnormalities with vaginal administration (19). In our investigation, uterine contractile abnormalities were more frequent in women treated with oral misoprostol, although the abnormalities did not differ significantly from those of women who received vaginal misoprostol. Less than 15% of women who received vaginal misoprostol had tachysystole, which is lower incidence in our experience as in other studies (22-24). The relatively long half-life of misoprostol and its metabolites in maternal serum after vaginal administration also might account for delayed tachysystole in women than those who received the medication orally (14). On the other hand, if we took into account the neonatal outcome, the oral dose was associated with a higher chance of admittance to the neonatal intensive care unit but this was not statistically significant. Our limited data supported the use of 50 mcg doses of oral misoprostol for preinduction cervical ripening and labor initiation because it had almost same efficacy and safety as its vaginal analogue. Oral route approach offered convenience, higher patient acceptance, ease of administration, and reduction of nursing interventions. In order to clarify the aforesaid side effects of misoprostol use, it appeared that the adverse effects were not only misoprostol related but it may be dose as well as dose interval dependent and probably has a large inter-patient variability in terms of pharmacokinetics. Conclusion Our results indicated that, in a closely supervised hospital setting with adequate monitoring, 50 mcg oral misoprostol has the potential to induce labor as safely and effectively as its vaginal route. Additional research is needed to categorically determine the most effective dosing regimens and intervals. We also believe further studies on safety with larger numbers of women need to be conducted before we advocate routine oral misoprostol. References
© Copyright 2009 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj09005t3.jpg] [mj09005t1.jpg] [mj09005f1.jpg] [mj09005t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}