 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
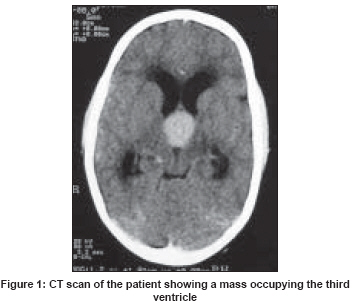
Neurology India, Vol. 56, No. 2, April-June, 2008, pp. 207-209 Letter To Editor Intraventricular adamantinomatous craniopharyngioma in a child Agrawal Ritesh, Misra Vatsala, Singla Meenakshi, Chauhan ShishupalC, Singh PremalaA Department of Pathology, Moti Lal Nehru Medical College, University of Allahabad Code Number: ni08058 Sir, Craniopharyngioma constitutes about 3% of brain tumors and commonly presents in the first or second decade of life. [1] Intraventricular craniopharyngiomas are rare and usually present in adults as squamous papillary type. A case of intraventricular adamantinomatous craniopharyngioma of the third ventricle in a child is documented here due to its rarity. A10-year-old female presented with history of headache for one year with diminution of vision in the left eye for two months. She could count fingers at two feet from the left eye. Right eye was normal with bilateral papilledema. There was no neurological deficit. On computed tomography (CT) scan, a well-defined, round, hyper-attenuating mass lesion, 2.31 x 2.48 cm, was present in the anterior part of the third ventricle without post-contrast enhancement and foci of calcification [Figure - 1]. Hydrocephalus was present. A preoperative MRI was not done due to lack of resources and poor financial status of the patient. Ventriculo-peritoneal shunt was done approximately 4 h before the planned surgery as an emergency procedure because the condition of the patient was deteriorating due to suspected herniation. The mass was excised completely by right transsulcal-transventricular approach via the right prefrontal sulcus. The mass was cystic and loosely attached with clear, oily fluid inside it. Histopathology showed glial tissue lined by cords, bridges, and nests of stratified squamous epithelium with palisading of basal nuclei at the periphery and spongy reticular-like stellate cells towards the base. At places, foci of compact keratin with ′ghost cells′ was also seen. No intracytoplasmic keratin or keratohyaline granules were seen. The surrounding brain tissue showed gliosis, chronic inflammatory cells and Rosenthal fibers [Figure - 2]. A diagnosis of adamantinomatous craniopharyngioma was made. Patient had improvement in vision at two months of follow-up. Intraventricular adamantinomatous cranio-pharyngioma is rare, especially in a child. Recently, a case of fourth ventricle craniopharyngioma from a child was reported supporting its ectopic origin. [2] Histologically, craniopharyngiomas are divided into two types: adamantinomatous and squamous papillary. The adamantinomatous type usually occurs in the first and second decade of life. The location is usually suprasellar, although it may occupy the sella as well. It is mainly cystic and is characterized by calcification, keratin nodules, cholesterol clefts and high recurrence rate. The squamous-papillary type predominantly found in adults is mainly solid and is characterized by a much lower incidence of calcification, keratin, recurrence, and brain invasion compared to the adamantinomatous type. [1] Intraventricular craniopharyngiomas were classified by Pascual et al., into strict intraventricular (34.3%) and non-strict intraventricular (65.7%) groups. [3] In the non-strict group, a preferentially adamantinomatous pattern with wider and tighter adherence to third ventricle margins was found along with a worse prognostic outcome. [3] Our case was strictly the intraventricular, adamantinomatous type but was loosely attached to ventricular walls. The main differential diagnoses considered were colloid cyst, epidermal inclusion cyst and Rathke′s cleft cyst which were ruled out by the morphology of the lining epithelium, absence of hyphae-like aggregates of degenerating nucleoproteins, intra-cytoplasmic keratohyaline granules and mucicarmine-positive goblet cells atop squamous epithelium. [4] Pierre-Kahn et al., removed 12 intraventricular craniopharyngiomas from children. Out of those, seven were removed totally. However, all suffered from hypothalamic syndrome. That lead the authors to suggest a radical removal for extra-ventricular craniopharyngiomas only. [5] We removed intraventricular lesion almost in toto that was confirmed by improvement in vision and other clinical parameters of the patient at two months′ follow-up. It could not be confirmed by a postoperative MRI due to the financial constraints of the patient. References
Copyright 2008 - Neurology India The following images related to this document are available:Photo images[ni08058f1.jpg] [ni08058f2.jpg] |
| |||||||||

{kind=link}
{kind=link}