 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 5, No. 16, Jan - March, 2006, pp. 938-940 Oral papilloma in pediatric patients Francisco Wanderley Garcia de Paula e Silva1* , Alexandra Mussolino de Queiroz2*
1DDS, Graduate student 2DDS, MSc, Professor *Department
of Pediatric Clinics, Preventive and Social Dentistry at the Faculty of Dentistry
of Ribeirão Preto, University of São Paulo, Brazil.
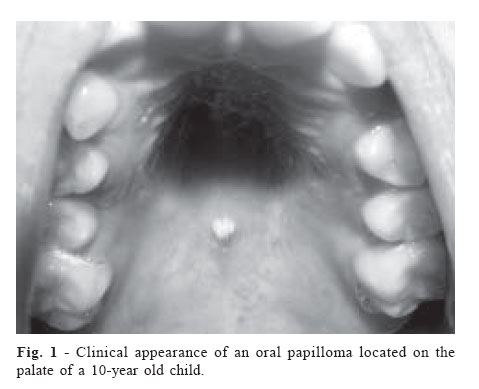
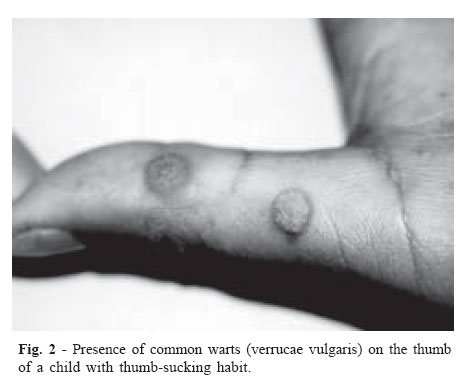
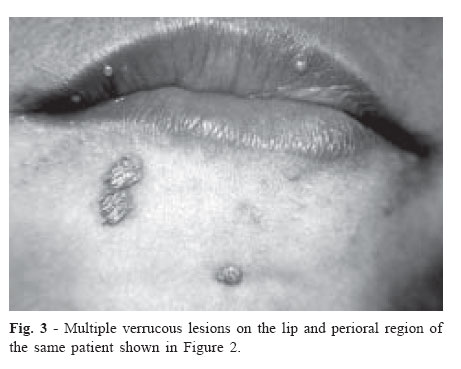
Received for publication: September 22, 2005 Code Number: os06001 Abstract Oral papilloma occurs relatively commonly intra-orally in pediatric patients who are usually unaware of their presence because this lesion is usually single, asymptomatic and small. The aim of the present study is to describe the clinical and histological appearance of this lesion and provide subside to help the general or pediatric dentist on diagnosis and treatment of this tumor. Key Words: oral papilloma, pediatric patient, dentistry Introduction Papilloma is a benign neoplasia of the stratified squamous epithelium, which is relatively common in children1-2. The findings of a study that reviewed data from 2,356 biopsies of young patients (birth to 14 years) received over 15 years in an Oral Pathology Service in Brazil revealed that papillomas were the most frequently observed benign tumors of non-odontogenic origin, corresponding to 29.5% of these lesions3. Al Khateeb et al.4, in a 10-year retrospective analysis of the types and distribution of oral and maxillofacial tumors in north Jordanian children and adolescents, reported that the papilloma was the most commonly found benign epithelial tumor in this population. Das and Das2, after reviewing the results from 2,370 biopsies of patients up to 20 years of age collected over 11 years in the biopsy service at the University of Illinois, USA, reported that the papilloma was the most prevalent oral neoplasia in this population. Although its exact etiology is still unknown, it is believed that the origin of papillomas is related to traumatisms or to human papillomavirus, especially HPV-6, 11, 16, which have already been identified in these lesions5. The theory that associates papillomas to the HPV advocates that this virus is capable of invading the nuclei of the cells in the spinous layer, inducing a series of proliferative alterations that result in tumoral growth6-7. The papillomaviruses are a heterogeneous group of over 100 deoxyribonucleic acid (DNA) viruses that are predominantly located in the squamous epithelium, causing hyperplastic, papillomatous and verrucous lesions in human and in a wide range of animals5,8. The possible modes of HPV transmission in children include vertical transmission, auto and heteroinoculation by genital, sexual or casual social contact5-6,8-9. In children younger than 1 year of age with papilloma lesions, maternal-fetal or maternal-neonatal HPV transmission is most likely involved. Intrauterine transmission may occur via hematogenous spread either due to recent infection or reactivation of a latent infection of the mother5-6,10-11. It has also been suggested that neonates could acquire the HPV infection due to aspiration of amniotic liquid as they pass through the vaginal birth canal during delivery. In children older than 1 year of age, HPV transmission may occur by both auto and heteroinoculation6. Moreover, the possibility of childhood sexual abuse should be considered when other routes of transmission (i.e., autoinoculation by hand to genital area and genital area to hand or mouth, nonsexual contact or perinatal transmission) have been ruled out6. In the oral cavity, papillomas most commonly occur on the palate (34%) (Figure 1) and jugal mucosa, but may also affect the uvula, tongue, lips and gingival1-2. These tumors are characterized by an exophytic, painless, well-delimited growth, and the numerous small digitiform projections on their surface give them a clinical “cauliflower-like”appearance1. Papillomas usually manifest as single, whitish lesions but may have the color of the surrounding mucosa. Although papillomas are typically small, generally measuring only few millimeters in diameter, there are reports of lesions measuring several centimeters12. Generally, the clinical appearance of oral papillomas is hardly distinguishable from that of common warts (verrucae vulgaris). For an accurate differential diagnosis, it is necessary that any HPV that is normally found in skin lesions also be identified in the intraoral lesion. The papillomaviruses present in skin lesions that have been associated to intraoral common warts are HPV-2 and 575. A logical association for clinical diagnosis would be to establish a connection between the presence of common warts in the child’s hands and fingers, habits such as thumbor finger-sucking and onychophagia, and the oral papilloma lesion6 (Figures 2 and 3). The histological examination of these lesions reveals the proliferation of the spinous layer cells, following a digitiform pattern with a delicate core of fibrous connective tissue constituting the supporting stroma12-13. Variable degrees of inflammatory reaction can be observed in this stroma, depending on the existence of epithelial ulcerations14. The treatment consists of complete excision of the base of the lesion and a small area of surrounding normal tissue using a number 15 stainless steel scalpel blade12. The specimen should be sent for histopathologic examination to confirm the clinical diagnosis of papilloma and to assure that the surgical intervention and treatment management of the pathology were adequately performed. References
Copyright 2006 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os06001f3.jpg] [os06001f2.jpg] [os06001f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}