 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
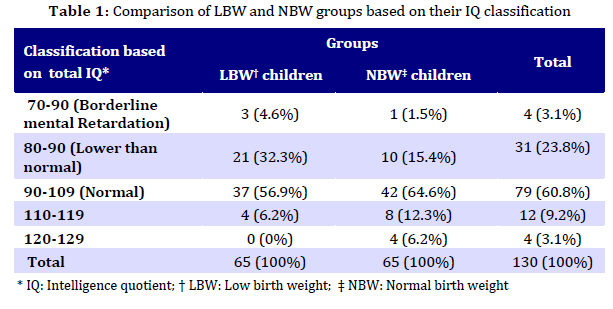
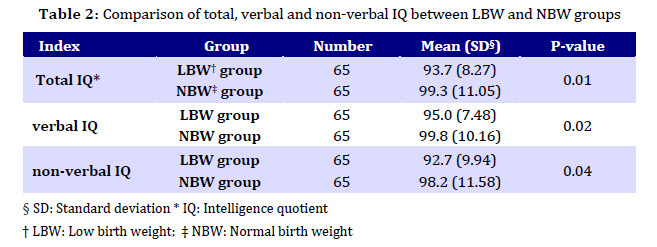
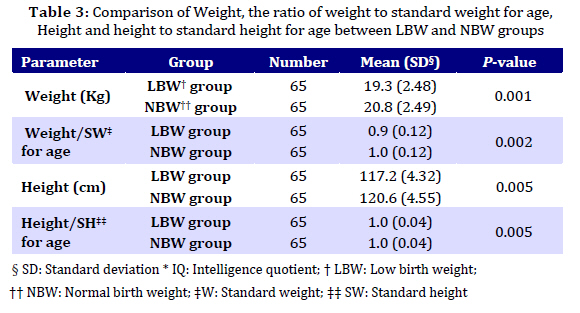
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 387-392 Intelligence Quotient (IQ) and Growth Indices in Children with the History of Low Birth Weight Manoochehr Mahram1, MD; Noureddin Mousavinasab2, PhD; Amin Gooran Urimei3, MD 1. Department of Pediatrics, Zanjan University of Medical Sciences, Zanjan, IR Iran * Corresponding Author; Address: Deputy for Health, Qazvin University of Medical Sciences, Mofatteh St. Mirdamad Blvd. Ghiath Abad, Qazvin, IR Iran E-mail: drmahram@yahoo.com Received: Dec 11, 2008; Final Revision: May 17, 2009; Accepted: Sep 06, 2009 Code Number: pe09046 Abstract Objective: In two groups of children with and without the history of low birth weight (LBW), Intelligence Quotient (IQ) and growth indices including weight and height are compared. Key Words: Low Birth Weight; Intelligence Quotient; IQ; Weight; Height; Children Introduction Newborns weighing 2,500 g or less at birth are known as LBW (Low Birth Weight), which may be caused by preterm birth, intra uterine growth retardation (IUGR) or both. These infants are in a higher risk for mental retardation, sensual, cognitive and developmental defects. At school age, these complications can be observed prominently in VLBW (Very Low Birth Weight = BW of 1,500 g or less) children, in the form of poor physical growth, cognitive function and school performance, which appear to persist into adulthood[1]. LBW as a classification includes premature infants (younger than 37 weeks gestational age) and term (37 weeks or older) infants who are small for gestational age (SGA). Many preterm infants are also IUGR when growth is based on fetal growth standards. These IUGR preterm infants are at increased risk for perinatal demise and neonatal complications. IUGR is the predominant cause of LBW in developing areas and nations with LBW rates greater than 10%[2]. According to World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) in 2004, about 15.5 percent of all neonates are born with low birth weight worldwide, 95.6 percent of which are in developing countries. The levels of LBW in developed, developing and least developed (undeveloped) countries are 7 percent, 16.5 percent and 18.6 percent, respectively. The incidence differs in different regions of the world as below: 14.3 percent in Africa, 18.3 percent in Asia (with a wide range from 5.9% in East Asia to 27.1% in South-Central Asia), 6.4 percent in Europe, 10.0 percent in Latin America and Caribbean, 7.7 percent in North America and 10.5 percent in Oceania. According to the national report of 1995, the incidence of LBW in Iran was 7 percent[3]. Spontaneous preterm labor, as the main cause of LBW deliveries, accounts for 40% to 50% of all preterm deliveries. Many of risk factors leading to preterm labor are preventable, such as infection, poor nutrition, anemia, smoking, alcohol abuse, heavy physical work, physical or psychological stress, inadequate prenatal care, etc. Furthermore, some maternal medical conditions and diseases such as exposure to diethylstilbestrol, diabetes and hypertension can be controlled [4]. In this study, to compare two groups of children with and without the history of LBW, Intelligence quotient (IQ) and growth indices including weight and height were measured. Subjects and Methods In this historical cohort study performed in Zanjan City (Iran), 130 six-year-old children of both sexes in two equal groups, 65 with LBW history and 65 with the history of normal birth weight (NBW), were selected randomly to be assessed for IQ and physical growth indices. Six-year-old children of both sexes with the history of LBW, referred to health centers for pre-school children, were simply randomized and included in the study as cases. Control group consisting of children with the history of normal birth weight were selected in the same manner. The information about the birth weight of the children was obtained from birth files rather than asking parents, and doubtful cases were omitted. Furthermore, children with the history of diseases affecting IQ or growth such as severe or prolonged neonatal jaundice, hypothyroidism, malnutrition, metabolic disorders, mental or neurologic diseases, handicapped children and so on were excluded from the study. To reach more accurate results, cases with birth weights between 2400 and 2600 gram were excluded, too. As much as possible, based on the information of the health files, we tried to exclude the children with the history of IUGR; so the cases with LBW history consisted of individuals with premature or SGA history. Although, some other variables such as socio-economic situation, may affect the results; these were ignored regarding the probability of differences in case and control groups. IQ was measured using Wechsler Intelligence Scale for Children-Revised (WISC-R) by experienced experts. Measurement of weight (W) was performed barefoot with the least clothing and by means of standardized Seca scales in kilograms, height (H) by means of a wall mounted "height measuring tape" in centimeters with the child standing barefoot and completely upright, heels, back and head touching the wall, and a straight plate on the head. Because of a little difference in age (around a few months) of the children in both groups, the quantities of W and H could not be compared accurately; therefore, we changed these quantities to the ratio of W or H to standard W or H for age, the nominator of these fractions was calculated based on following formulas: Standard W (Kg) for age 7-12 yr-old=age(yr)× 7-5/2, Standard H (Cm) for age 2-12 yr-old=age(yr)×6+ 77[5]. The results of the study were analyzed statistically using SPSS (Statistical Software for Social Studies) software, t-test and Chi-squre. P-values less than 0.05 were considered as significant. All ethical aspects were considered in this study. No expenditure was imposed on the cases and all the personal information was considered confidential. Findings Study population consisted of 65 children with the history of LBW (32 males and 33 females) and 65 with the history of normal birth weight (33 males and 32 females). Mean birth weight for LBW and NBW children was 1.885±0.337 Kg and 3.200±0.368 Kg, respectively. The results of measuring total IQ and the classification of the cases based on the number of total IQ are shown in table 1 and comparison between the two groups, based on total, verbal and non-verbal IQ is shown in Table 2. Comparison of weight and height between the two groups showed significant difference in both parameters. Furthermore; comparing two other important variables, ie the situations of weight (as the ratio of weight to standard weight for age) and height (as the ratio of height to standard height for age), between the two groups, showed significant differences in both parameters (Table 3). Discussion Regarding results of the study, LBW delivery affects verbal, non-verbal and total IQ, weight and height in the children significantly, compared to those having a history of normal birth weight. These results were similar to the findings of Chaudhari et al (P=0.006)[6], Kitchen et al (P<0.05)[7], Emond et al (P=0.04)[8], Breslau et al[9,10], McCarton et al[11], Hack et al[12] and Elgen et al[13] who compared verbal, non-verbal and total IQ between two groups of children having LBW history and a control group and found significant differences. Sommerfelt et al found a significant difference in non-verbal component of IQ between the two groups (P=0.005), and although verbal component was lower in LBW group, the difference was not significant. This was different from our finding. The researchers believed the reason was a better nurture in LBW group in their study, as higher family income and childrearing factors were stronger predictors of verbal IQ[14]. Roussounis found significant total IQ difference between boys and girls of two case and control groups[15]; which is similar to our findings. Bhutta et al conducted a meta-analysis of studies on the cognitive and behavioral outcomes of school-aged children who were born preterm and found reduced cognitive test scores and the risk of some behavioral disorders, such as ADHD[16]. Some studies have demonstrated more careful results about the relationship between IQ score and birth weight. Matte et al found out that IQ in boys predicted about 0.5 points difference per 100 gram change in birth weight (95% CI, 0.28-0.71), but not in girls[17]. Tong et al found a statistically significant association between birth weight and cognitive performance at age 2 years (adjusted deficit: 0.97 points per 100 g lighter; 95% CI: 0.4–1.5), but the magnitude of this association gradually decreased and became statistically non-significant at later childhood[18]. In addition, our results showed significant difference in mean weight and height between two the groups (P=0.001 and P=0.005, respectively). This significance was observed in both "the ratio of weight to standard weight for age" and "the ratio of height to standard height for age", too (P=0.002 and 0.005, respectively). These results are similar to the findings of Emond et al[8], Elgen et al{13}, Clarkson et al[19], Peng et al[20], and Cooke et al[21]. Bjere although found lower weight and height in LBW children than in the control group, this difference was not significant[22]. The important limitations in our study were: 1) absence of reliable information on the gestational age in some of health files to differentiate prematurity from IUGR, 2) some parents as the source of information about the history of their children were not oriented and careful enough to give accurate history, 3) Probability of some differences in environmental factors including socioeconomic situation, childrearing styles and so on among individuals in the two groups. Although we ignored the third point, the first two made us exclude a few children and replace them with other cases. Conclusion The results of this study and similar studies indicate the importance of intrauterine physical and brain growth, and its effects on intelligence and growth indices in later years. Furthermore, these emphasize on paying special attention to: the problem of low birth weight deliveries, recognizing the related risk factors, and trying to reduce them. Acknowledgment This study, as part of thesis of Dr. Amin Gooran Urimei, was supported by a grant from Deputy for Research Affairs of Zanjan University of Medical Sciences, for which we thank. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09046t1.jpg] [pe09046t3.jpg] [pe09046t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}