 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 2, Apri l-June, 2011, pp. 193-200 The Effect of Parental Presence on the 5 year-Old Children's Anxiety and Cooperative Behavior in the First and Second Dental Visit Hossein Afshar1, DDS, MS; Yahya Baradaran Nakhjavani1, DDS, MS; Javad Mahmoudi-Gharaei2 MD; Mehrsa Paryab3, DDS, MS; Sommaye Zadhoosh4, MA
Received: Feb 25, 2010; Final Revision: Aug 31, 2010; Accepted: Dec 26, 2010 Abstract Objective: One of the most significant problems in pediatric dentistry is behavioral resistance of preschool children in the first visit. There is a debate on parental presence in operation room. The purpose of this study was to evaluate the Iranian 5-year-old children’s behavior including anxiety and cooperation relative to parental presence in the first and second dental appointments. Key Words: Parental Presence; Anxiety; Cooperation; Behavior; Rating Scale Introduction Pediatric dentistry, along with developing suitable oral health among children, attempts to provide, simultaneously, a positive outlook in children following a dental visit. It, therefore, tries to manage the children’s anxiety and fear utilizing different techniques. Techniques, such as providing information, Tell-Show-Do, Reinforcement, Relaxation, Distraction, and Parental Involvement are used for better interactions. More invasive techniques, such as Voice Control, HOM (Hand over mouth), and Physical Limitations to reduce the probable inappropriate behavior of the child during the visit are also used[1,2]. Following the social changes today, less aggressive methods are more acceptable to children as well as to their parents. The most widely used technique among the pediatric dentists, which is also less invasive, is the parental presence/absence. In this technique, the parents are present in the dental operation room, and in case the child is uncooperative, the parent is asked to leave the room, and after the cooperation is stabilized, and as a reward, the parent is again asked to be present in the room[3]. Kotsanos, et al observed the success of this technique during the first and successive treatment visits[4]. The increasing persistence of the parents for presence near their children[5,6] has made dentists to re-evaluate their strategies for asking the parents to leave the room. Psychiatric researches have confirmed the presence of at least one of the parents in order to enhance feeling of security and betterment of the child’s behavior[7]. The studies conducted in dentistry in different nations and cultures have been unable to demonstrate similar conclusions[8-13]. The results of the study by Frankle, et al demonstrated a positive impact for the parent’s presence[10]. In 1967, Croxton obtained positive successful clinical results in treating 28 children aged 3-12 years. The children had been referred due to behavior problems which were related to their separation from their parents during dental visits. He noted that parent’s presence increased the children’ behavior problems, and hence resulted in the failure of the dentist in managing the child[10]. Marzo, et al concluded that there had been better results obtained in the group of children whose parents were absent, and patients’ absence were reduced for the second visit[8]. However, the results of more other studies revealed the lack of parental influence on children’s behavior. Lewis and Law in 1958 were unable to obtain meaningful statistical differences in psycho-physiologic reaction to parental presence in children with a previous dental visit[11]. In 1978, Venham, et al studied the reactions in 64 children aged 2-5 years (30 boys, 34 girls) without any prior dental visits in the two groups of with/without parental presence. The visits included preliminary visit, diagnosis, and prophylaxis and fluoride therapy. During the treatment phase, the children’s heart beat rate, baseline skin reaction, or skin resistance to electrical current were observed followed by Venham Picture Test at the beginning of each visit with scaling the clinical behavior and anxiety via taped Films using Venham Anxiety and Behavior Scale. Total and one-by-one visits session studies did not reveal any significant differences in children’s reactions with/without parental presence[12]. The same results were repeated in their 1979 study[9]. Pfefferle, et al studied behavior in 48 children (36-60 months old) who had no prior dental visit experience. Their study was done using North Carolina Behavior Rating Scale (NCBRS). No significant differences were found between parental absence/presence[13]. Still in other studies, like the one conducted by Fenlon, et al, who studied behavior in 31 British children (<12 yrs old) based on Franckle Scale, it was found that parents’ presence/absence has no impact on child cooperation[10]. Bearing in mind that the results of the researchers in different nations have not reached any consensus regardless of their different techniques used, the present study was designed to observe the parents’ presence/absence in dental visits in Iranian 5-year old children. Subjects and Methods This randomized clinical trial study (with control and study groups) approved by ethics committee of Dental Research center of Tehran University of Medical Sciences and was conducted on sixty seven 5-year (±2 months) olds presenting at the pediatric department of dental school in 2009. The inclusion criteria were as follows:
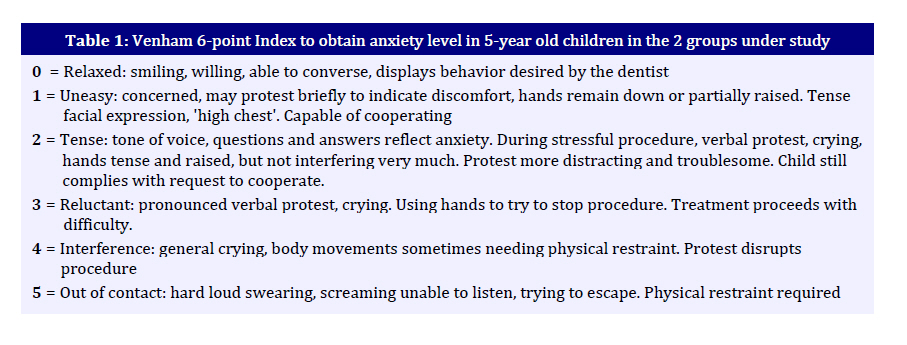
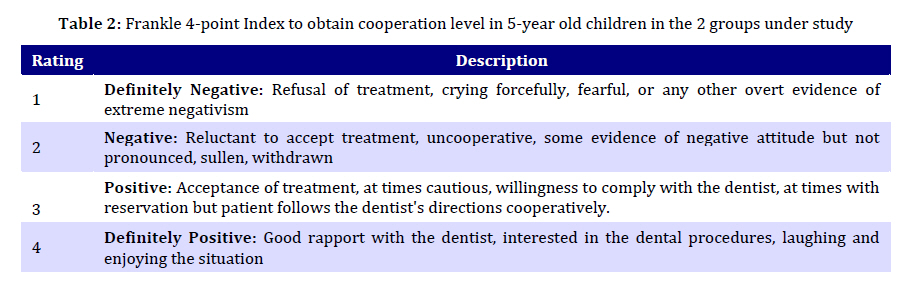
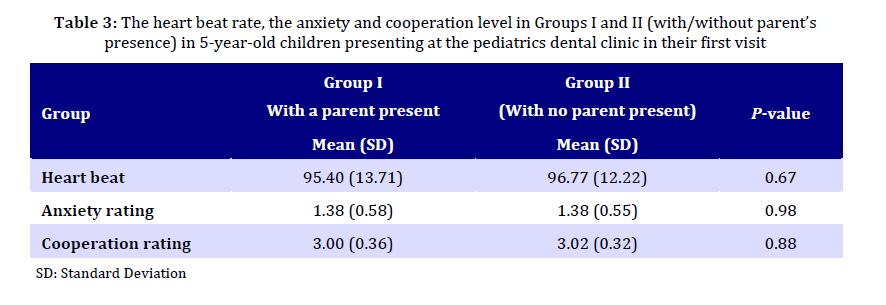
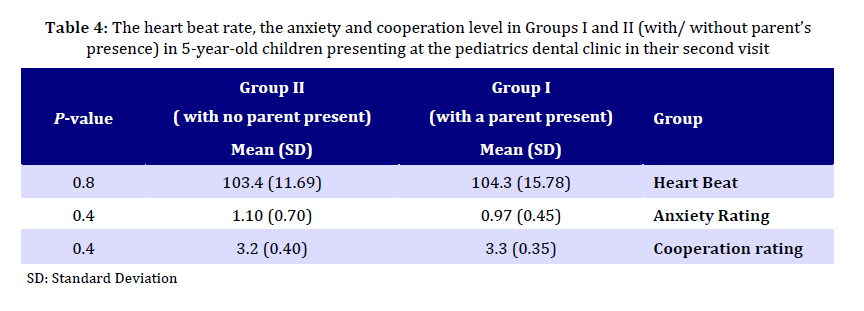
Prior to any visit by the dentist, the parents were asked to sign a consent form and a questionnaire covering 4 parts of parents’ and children’s demographic and social information along with the parents’ opinion on their own presence in the room, as well as their prediction of their child’s behavior during the visit. The selected children were assigned into 2 groups by even-odd method. The first group (Group I), included those whose parents were present; while the second group (Group II), included children whose parents were absent. In the operation room, the mother’s seat was chosen to be on the right hand side of the dental chair (but out of the sight of the video-camera vision). The mother was asked not to talk to either the child or the dentist during the visit. She was also asked not to interfere in any form in case the child was not cooperative. The video-camera was on as soon as the child entered the room. It was located on the top of the dental unit light pole and was positioned to show the child’s head and hands. The dentist started by asking the child his name and age; then by the Holst Technique, he tried to manage his behavior which included Tell-Show-Do, clinical visit, prophylaxis with paste and rubber cap and fluoride therapy. After prophylaxis and at the beginning of fluoride therapy, the child’s heart beat rate was rated by the dentist by hand. At the end of the first visit, the necessary radiographies were prescribed for the child and the date of the second visit was set. Of the 67 children visited at the first session, 56 required a second visit. 8 of these children did not show up. The parents’ presence in the second visit was similar to that in the first visit. 24 children were with their parents, while 24 others were alone and without their mothers in the operation room. In the second session, following describing what the child had to undergo (which included a simple and easy-to-understand method), the required injection and treatments were performed. It was tried to include similar treatments for all children including a mandible plaque injection, and pulpotomy treatment of a molar deciduous tooth, which was done on 42 of the children. The rest 6 of the children required amalgam treatment and composites. It should be noted that the treatment procedures in the two groups followed a normal distribution. The heart beat rate of each child was recorded following injection. In both sessions and in all children, parameters such as the attending dentist, his assistant, the working environment, time and duration (30 minutes for each child) of work, and the type of dialogues were all constant. Care was taken to make sure that the children were not tired, hungry, or having cold. The quantification of the children’s behavior upon the taped films was based on Venham Scale: for anxiety level (Table 1); and for behavior level, it was based on Frankle Index (Table 2). The ratings were performed by 2 separate pediatric dentists who were blinded on the procedures of the study. Finally, mean values of the results of ratings were used for data analyses. SPSS 15 was used for t-test and ANOVA in data analyses. Moreover, regression analysis was used for the impact of the baseline variables on cooperation and anxiety to adjust the interfering variable (parent’s presence/ absence). A P<0.05 was considered as meaningful. Findings The patients in our study were 33 boys and 34 girls (n=67) in the first visit of whom 32 were in Group I (with their parents present), while 35 patients were assigned in Group II (without parents being present). Data analysis revealed that both groups followed similar patterns for their sex, parental education, parental dentistry experiences, number of children in the family, and going to kindergarten. Table 3 shows the mean and standard deviation (SD) for the heart beat rate, the anxiety level, and cooperation in the first visit in both groups. As it can be seen, heart beat rate, anxiety and cooperation level show no significant differences (P value>0.05) (Table 3). Table 4 depicts the mean value and SD for heart beat rate and cooperation level as well as their anxiety in the second visit in both groups. For the same variable, no significant difference was found. Moreover, there were no significant differences for the anxiety level and cooperation between the two groups during study (P>0.05) (Table 4). Discussion Doubt on the parents’ presence/absence in a social experience like dentistry visit, and its probable impact on child behavior has caused research in this area. The present study was therefore, designed to scrutinize the issue among Iranian children who are educated with their native culture. The study exclusively included 5-year-old children. Based on Piaget’s classification, these children are in the recognition phase of pre-operational phase. Their vocabulary increase, attention, and concentration are signs of their readiness for social experiences[14]. At this age, the children demonstrate more stable behaviors[15], with fewer possible and unpredictable negative behaviors than the children 4 years old[10,15]. Moreover, it has been shown that maternal anxiety and the child’s temperament have lower impacts on child’s behavior[16,17]. At the same time, the child has not yet entered society, showing that he/she is more under the cultural-educational condition than being under the influence of different social experiences. In most studies[9-13], it has been revealed that the children entering schooling are not comparable with pre-school children. It has been known that a collection of parameters can cause anxiety and behavior problems in children (along with age as still another parameter) during a visit in a dental clinic[17]. In line with other studies, the children in our study did not have any previous visits to a dentist nor did they have any history of severe dental pain, nor any systemic disease and hospitalization. In our study, parents were asked on any delay in the physiological development with previous familial problems as well as harmful events and severe fear from strangers, or any visits to a psychiatrist, as it has been noted that such variables can enhance negative behaviors in children[16-20]. The parent’s presence/absence in our study during the first and second visit was chosen randomly which has been similar to that of Pfefferle, et al (1982) as well as that of Fenlon, et al in 1993[10, 13]. However, in the study by Venham et al (1978), the parent’s presence/absence was decided based on the parent’s desire, or that of the child’s. Moreover, the parent was allowed in case anxiety shown by the child[12]. In the next study of Venham et al (1979), the children were randomly assigned into either of the groups of parent’s presence/absence during the first visit, while for the second visit, the reverse procedure was used[9]. It seems that parent’s presence/absence upon child’s request, or even that of the parent’s, had been influenced by the dependency or independency on the part of the child, causing behaviors assessing more the individual’s psychological manners. The procedure in the present study was in line with most other previous studies including Holst Procedure[8-13]. Based on the obtained results, this technique enhance a positive reaction and acceptance of the treatment procedures[18,20,21]. In our study, however, the cooperation and anxiety levels were assessed separately with 2 different methods which was in line with the method used by Venham, et al[9,12], while in other studies[8,10,13] only the level of child’s cooperation had been evaluated. Since disrupted behaviors and lack of concrete clinical cooperation can occur without any anxiety for dental visits, it seems reasonable to study each of the variables (including parent’s presence) separately[22]. In evaluating anxiety and cooperation levels, we used physiological and behavioral indexes. As physiological indexes alone have not been successful in assessing anxiety[11], we considered simultaneous behavioral observations, and it seems that these indexes are more suitable in assessing 5-year old children, because these children at pre-school age have less power to demonstrate their feelings which are even more reduced in stressful circumstances. Moreover, the results of parents’ evaluations are not always parallel with the obtained results[23]. The physiological index in our study included the heart beat rate. It has been shown that this index is more in line with the anxiety experienced in dental visits[11,24-26]. The most appropriate method for assessing child’s behavior in a dental visit is the recording of the behavior through a video-camera, and then quantification of his/her reaction by an unaware observer (the blind method), as well as using a scale[9]. The scales used in our study (for quantification) was that of Frankle and Venham Scales. Frankle index has been widely used in numerous studies [4,10,19,27]. Fenlon et al (1993), have shown its reliability to be 100% [10]. Venham index includes 6 levels (0-5), and is very easy and quick with a reliability and validity for statistical analyses. The homogeneity of the results obtained through this scale by different observers has been reported to be between 0.78-0.96 [9,12,24,25,28,29]. In short, the results of this study have shown that the parent’s presence/absence has no impact on the anxiety and behavioral level of the children 5 years of age during the first and second visits. Our results are totally in line with the results obtained in the 1958 study by Lewis and Law[11], 1968 study by Allen and Evan[10], Venham et al (1978, 1979)[9,12], as well as the 1982 study by Pfefferle et al[13], and 1993 study by Fenlon et al[10]. Considering the exactness of the procedures used in our study, including limiting the age range, having the same dentist throughout the study, random sampling of the parent’s presence/ absence, and selecting the children based on more interfering parameters, it seems that the results of the present study are more applicable to Iranian 5-year-old children. Our results are, however, different from the results obtained by the 1967 study by Croxton[10], and 2003 study by Marzo et al[8]. Croxton had studied children who had had an unfavorable dentistry experience, and Marzo et al, used a 2-level scale for assessing the cooperation level. It seems that their results are less useful for documentation. Bearing in mind the similarities and differences of the present study compared with other studies, it seems that most Iranian 5-year-old children, with their education and Iranian culture, can have a positive dental visit without experiencing a lot of anxiety and lack of cooperation even when their parents are absent. This is in line with Jean Piaget’s theory stating that children at this age can tolerate separation from parents, enhancing self-confidence, and self-control as well as obtaining social experiences when facing strangers without any affective consequences[14]. Moreover, in cases where parents request to be present in the operation room, it can be predicted that their presence has no negative impact on cooperation and anxiety of their children. In addition, it seems that a previous unfavorable medical or dental visit plays more important role than the parent’s presence/ absence or the number of visits, so that in case of using the Tell-Show-Do procedure for an Iranian 5-year-old child with his/her Iranian method of education in the first visit, it can be expected that the child would feel comfortable, and be without any affective consequences, or behavioral problems in dental treatments, if a positive imagination is formed in the child, regardless of whether the parents are present. The nature of this data is descriptive and any conclusions reached should be restricted to the actual test population. An inability to use a scientific sampling scheme to obtain the test sample limits the degree to which these subjects are representative of a general population. Conclusion The parent’s absence/presence in the dentistry operation room has no impact on the cooperation and anxiety of the 5-year-old Iranian children who have had no previous dentistry presentation in neither the first nor the second visit. Considering our obtained results, it can be suggested that the parents be present during the first and second dental visits. The child’s reaction to the new environment (when the mother is present) can be evaluated and then the strategies for the successive sessions can be discussed with the parents. We do suggest further investigations on the children in other age ranges including children at 4 and 6 years of age. Acknowledgment This article is based on a postgraduate thesis submitted to the dental college of Tehran University of Medical Sciences. We would like to thank Dr. A.R. Shamshiri and Mrs. E. Danesh for their cooperation in preparing this work. Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11033t2.jpg] [pe11033t3.jpg] [pe11033t4.jpg] [pe11033t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}