 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
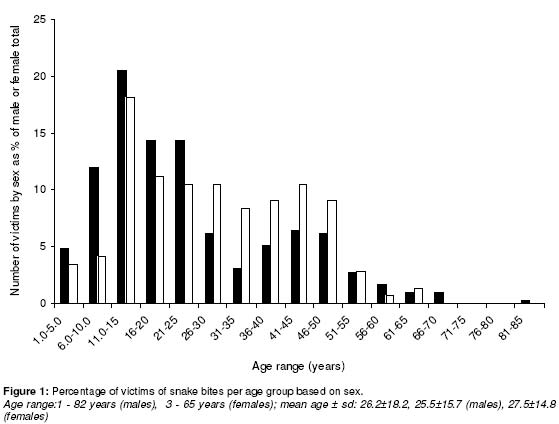
Tropical Journal of Pharmaceutical Research, Vol. 1, No. 1, June, 2002 pp. 39-44 Snake bites in Nigeria: A study of the prevalence and treatment in Benin CityEric K. I. Omogbai†, Zuleikha A. M. Nworgu, Michael A. Imhafidon, Anwakang A. Ikpeme, David O. Ojo and Charles N. Nwako Department of Pharmacology & Toxicology, Faculty of Pharmacy, University of Benin, Benin City, Nigeria Code Number: pr02006 ABSTRACTPurpose: Although snake bites occur frequently in Benin City, the prevalence has not been documented. This study was therefore done to determine the prevalence, morbidity, mortality, and the orthodox treatment of victims. Key words: Snakebite, prevalence, treatment, Benin City. INTRODUCTION Snakebite is a common occurrence in Nigeria as indeed in many parts of the tropics. The incidence and type of snake seem to vary according to the geographical zone, the occupational practices of the population and the season. It has been observed that the incidence of snake bite is seasonal and there is a peak during the rainy season - a time when frogs and toads emerging from their hibernation are preyed on by snakes that thereby come in frequent contact with humans,and when farmers engage in intense farming activities that also bring them frequently in contact with snakes in the bush1,2 . Venomous snakes are found throughout most of the world and are believed to cause in excess of 3 million bites per year with more than 150,000 deaths3. The venomous snakes in Africa are known to belong to four main families - the colubridae, elapidae, viparide and hydrophidae4 -but in Nigeria, the most common poisonous snakes are the elapids and viperids5. These include the Naja melanoleuca (black cobra) and N. nigricolis (spitting cobra), and the viperid Echis carinatus (carpet viper) and Bitisarietans (puff adder). Although most of the offending snakes reported in a study carried out in Zaria (a City located in northern part of Nigeria) were not identified, 69.6% of those identified belonged to the viperidae family while 30.4% were cobras (colubridae)1. Snake bites, are however, not confined to bush encounters as a significant numbers of victims are known to be bitten in their abodes; some while sleeping indoors. Itis known that snake bites occur frequently in Benin City, which is located in the tropical rain forest belt of South Western Nigeria, but the incidence has not been documented despite the fact that the condition is a recognized medical emergency. This retrospective study has therefore been done to determine the prevalence and the drug treatment of victims. PATIENTS AND METHODOLOGYThe study was done retrospectively in University of Benin Teaching Hospital, (UBTH) and Central Hospital in Benin City (CH) over a twenty-year period (1980-1999). Bothhospitals are tertiary health care centres; UBTH is a 550-bed Federal government-owned hospital while CH is a 500-bed State-owed referral health care centre. All patients treated for snake bikes in UBTH (226 patients) and CH (209 patients) from 1980 to 1999 were included in the study. Basic data such as the hospital number, cause for admission as well as the dates of admission and discharge for each case were obtained from the general records kept in the hospitals and the information was used to trace the relevant case files in the records archives from which the necessary data were collected. In extracting data from the case notes, special attention was paid to the age and sex of each victim, the part of the body bitten, the treatment given and the length of stay in the hospital, if admitted. The collection of data was done in two phases: the data spanning 1980 to 1990 were compiled in 1994 while those of the 1991 to 1999 period were collected in 2000. The data collected were then pooled and analysed in this report. The means and standard deviations were calculated for ages and durations of stay in hospital and where necessary, the Student t-test was used to compare the means. At 95% confidence interval, p-values less than or equal to 0.05 were considered to be significant. RESULTSA total of 435 cases comprising 292 males and143 females were recorded in the twenty-year period. Figure 1 shows the age and sex distribution of the victims. The overall mean age of victims was 26.2±18.2 years while the mean ages of male and female victims were 25.5±15.5 and 27.5±14.8 years, respectively. The youngest male and female victims were one and five years old respectively while the oldest male and female were 82 and 65 years respectively. The age of greatest vulnerability appears to be the teenage years and early twenties (Figure 1). There was no significant difference in the average ages of the male and female victims. Therecords showed that bites were frequently inflicted on the limbs; the right foot (41.8%), left foot (31.7%), right arm (14%) and left arm (6.9%). Bites on other parts of the body and spraying of venom into the eyes were also recorded (Table 1). Majority of patients, 259 (59.7%), were bitten in the bush, farm or on the road, and a significant number, 164 (37.7%), were bitten while outdoors around theirhomes while 12 (2.8%) were bitten inside their houses (Table 1). Table 1: Common sites and places of bite
Table 2 indicates the duration of stay of patients in the hospital. Of the total of 435 patients recorded in both hospitals, 397 were accounted for with regard to the duration of stay in the hospital. For the remaining 38 all of whom were recorded at CH, there was no indication as to their duration of stay. The records showed that 70 patients (16.1%) were treated and discharged the same day. The longest staying patient was in the hospital for 23 days. The mean duration of stay by victims in hospital was 5.7± 5.1 days. Table 2: Length of stay of patients in hospital
Duration of stay (days, mean±sd) = 5.7±5.1 Thedrugs commonly used for the treatment of victims are shown in Table 3. Two hundred and ninety-seven victims (68.3%) received antivenom(polyvalent) treatment while 67.4% receivedantibiotics. The most commonly used antibiotic agent was ampiclox® while others that featured in clu ded am picillin, metronidazole, gentamycin, benzylpenicillin, procaine penicillin and cotrimoxazole. Approximately equal numbers of patients received antihistamines (23.2%) mainly promethazine and chlorpheniramine and corticosteroids (23%). Twenty-nine percent weretreated with adrenaline, 82.5% received antitetanus toxoid, 61.5% received analgesics while 17.2% were given diazepam. Some of the patients (28%) received chymotripsin and 82.3% of the victims received intravenous fluids. One patient received Vitamin K for spontaneous bleeding. The site of bite was commonlytopically disinfected with hydrogen peroxide, gentian violet or chlorinated lime and boric acid solution. Table 3: Treatment profile of the victims
DISCUSSION It is known that snake bites in many parts of the tropics (especially the developing countries) are treated either by traditional healers at home or by orthodox practitioners in hospitals such that many cases are not reported to the hospital unless the traditional healer has failed to effect a cure and the victim survives to be taken to a hospital6. Hospital records may therefore not fully account for the prevalence of snake bites in the community. In Benin City however, the two major health health care centres have been surveyed in this study to obtain an approximation of the prevalence of snakebites in the city. In this study, the ratio of male to female victims is approximately 2:1 as against the generalpopulation ratio of approximately 1:17. This suggests that males are twice more likely to be bitten than females. This may be due to thefact that males are more adventurous and are therefore liable to have more frequent encounters with snakes. Some victims were bitten even indoors, indicating that people of all ages are potential victims despite the fact that the records show that the youngest and oldest victims were males. The intensity of exposure and bite frequency for both sexes appear to be highest in teenage years and in the early twenties - the most physically active years with the least amount of caution. Most bites were inflicted on limbs and there is evidence of a dextral predominance. The fact thatmost individuals favour the right hand and right foot and are therefore more likely to reach out or probe first with the right may account for this. Many patients appear to have been treated and discharged on the first or second day. This would be the case of bites with little or no envenomation in which there may be few or no symptoms. Even in cases of envenomation withdelayed reaction, the severity would have been known by the second day to enable a decision to be taken whether to discharge or keep the patient. The treatment profiles show that over 90% of patients were given tetanus antitoxin and/or tetanus toxoid. Tetanus prophylaxis is essential in snakebite because of the nature of the bites (puncture wounds) and the fact that snakes carry pathogenic organisms including Clostridium tetani as part of their normal oral microflora5. This predisposes victimsof bites even of non-venomous snakes to the danger of developing tetanus subsequently if not treated. This, along with the risk of infections by other pathogenic bacteria, justifies the use of the antibiotics identified in this study. While the penicillins are safe and useful for tetanus prophylaxis6, otherantibiotics as recorded in this survey are also useful for preventing or combating bacterial complication. There was no recorded case of tetracycline use in this study although our unpublished data of general antibiotic prescriptionpatterns in the two hospitals show a 3.1% use of tetracyclines. Tetracyclines are usually avoided in snakebite because of the risk of aggravating the acute renal failure which may occur with severe snake bite poisoning8. All patients who apparently showed signs of envenomation (68.3%) received antivenom (polyvalent in all cases) since, from the records, many of the snakes were usually not killed or identified but even when identified, specific antivenom is usually not readily available. When antivenom is used in the treatment of snakebite, hypersensitivity reactions are common and these usually warrant the use of adrenaline and corticosteroids and sometimes antihistamines. Early severe local tissue swelling, inflammation and haemorrhagic manifestations accompany viper bites and similar reactions have been reported for spitting cobra bites.2,3 It was observed in this survey that chymotrypsin has been used frequently as an adjunct in the treatment of caseswith tissues oedema and inflammation. Supportive fluid treatment may be advisable when shock is severe while the administration of a sedative like diazepam may be used to control pain and anxiety the latter of which could be pronounced even when there is no envenomation. Fear tends to complicate the treatment of snakebite as people have been known to suffer from shock after being bitten by non-poisonous snakes4. Diazepam is however not recommended in the treatment of victims of elapid snakebites with venoms that cause muscle paralysis and eventual respiratory failure in order not to exacerbate the paralysis. A surprising observation in this study, despite the high morbidity indicated by cases of prolonged confinement in the hospital of many patients, is the apparent absence of mortality. Although the fate of 8.7% of the victims was not recorded, no mortality was indicated. In a study of snake envenomation in children covering a period of ten years, LoVecchio and DeBus9 recorded no mortality among sixty-six victims of rattlesnake bites in a metropolitan area of Arizona in the United States and Chen et al recorded no mortality among 130 victims of poisonous snake bites in northern Taiwan during a 3-year period 10. However,the global mortality rate from snake bites appears to be about 5% of the victims.3 Ogala and Obaro1 reported a 3.9% mortality rateamong children bitten by snakes in Zaria, Idoko and Ibekwe11 recorded a mortality rate of 5.7% in 175 cases recorded in a two-year period in Makurdi, Nigeria while other researchers have also reported low mortality rates among victims of snake bites in different 13, 14 parts of the tropics.12, It has been suggested by these and other researchers that snake bites in the tropics are mainly "escape" bites in which only small amounts of venom are injected into the victims as against "business" bites in which large volumes of venom are injected.14, 15 It is also likely that the patients were usually brought early to the hospitals and had adequate and prompt care these being tertiary/tertiary and the best-equipped public hospitals in Edo State. CONCLUSIONIn conclusion, snakebite cases presented to the hospitals in Benin City were more common among males. Victims are more likely to be teenagers and youths in their twenties. While bites were more common outdoorspeople were also vulnerable indoors. The hospitals seem to have established adequate and effective treatment regimens for snake bite victims as no mortality was recorded during the period surveyed. ACKNOWLEDGEMENTSThe authors are grateful to the Chief Medical Directors of the UBTH and CH for providing access to their records for the purpose of collecting data for this study. REFERENCES
Full text of this journal is also available online at http://www.tjpr.freehosting.net © 2003 - Pharmacotherapy Group, Faculty of Pharmacy, University of Benin, Benin City, Nigeria. The following images related to this document are available:Photo images[pr02006f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}