 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Research Article Aqueous solubility of ciprofloxacin in the presence of metal cations Chukwuenweniwe Jonathan Eboka* and Henry Akpobor Okeri Department of Pharmaceutical Chemistry, Faculty of Pharmacy, University of Benin, Benin City, Nigeria Code Number: pr05004 Abstract Purpose: Though the complexation of ciprofloxacin
with metal cations has been extensively studied, the effect of this complexation
on the aqueous solubility of ciprofloxacin which is an important factor
affecting drug distribution has not been well documented. We have thus
set out in this study to investigate the aqueous solubility of ciprofloxacin
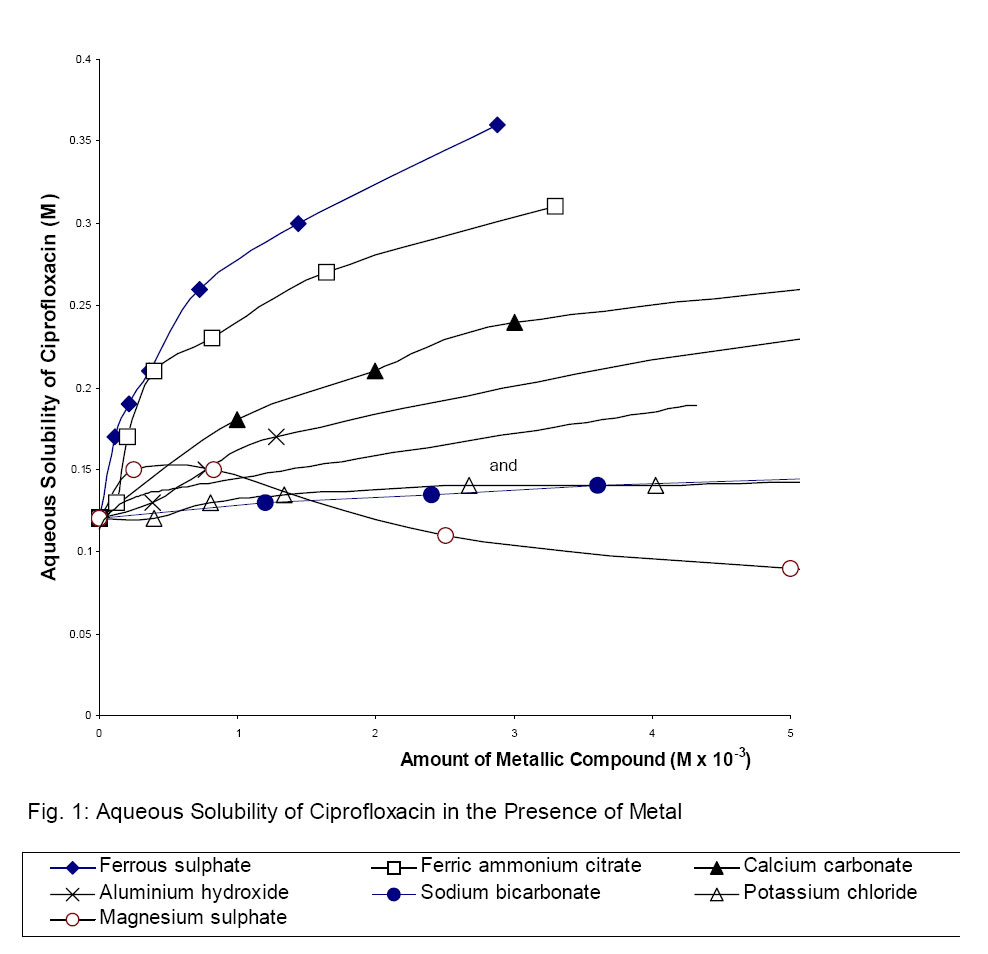
in the presence of metal cations. Key words: Ciprofloxacin, aqueous solubility, ciprofloxacin –metal cation interaction, antibacterial activity, gastrointestinal absorption. Introduction Ciprofloxacin is a member of the fluoroquinolone class of synthetic antimicrobial agents that has broad spectrum of activity against both Gram-positive and Gram-negative organisms (1). It is rapidly and relatively well absorbed from the oral route, penetrates and distributes well into tissues and thus reaches concentrations in serum, body fluid and tissues well above the minimum inhibitory concentrations (MICs). (2 - 4) Despite these desirable pharmacokinetic nd antimicrobial profiles, it has been observed that co-administration with magnesium- and aluminium- containing anti-acids resulted in nearly complete loss of activity. Reduced bio-availability was also reported when it was co-administered with preparations containing iron and multivitamins containing zinc (5 – 11). Different metal cations have also been found to reduce its antibacterial activity to varying extents in-vitro (12 –14). Because ciprofloxacin is widely used to treat resistant microbial infections (15), there has been obvious concern about its interaction with metal cations and how this affects its bio-availability and antimicrobial activity when they are co-administered. Such concomitant administration may not be avoidable. Several reasons ranging from complexation of ciprofloxacin with cations in the gut thus reducing its enteric absorption (5, 9), formation of insoluble, unabsorbable and antibacterially inactive chelate complexes, to formation of complexes which are less able to be taken up by bacteria than the free drug have been suggested to explain the observed effects. In all these considerations, the gastric absorption of ciprofloxacin, its tissue penetration and its penetration of the bacterial cell wall are important factors affecting its bio-availability and antimicrobial activity. The complexation of ciprofloxacin with the metal cations and how this complexation affects ciprofloxacin bioavailability and antimicrobial activity have been extensively studied. (16 – 24) However, it is not still clear how ciprofloxacin –metal cation interaction can account for the biopharmaceutical observations. We have therefore set out in this study to investigate the aqueous solubility of ciprofloxacin alone and compare it with its solubility in the presence of compounds containing various metal cations used in pharmaceutical practice and at a simulated pH of the stomach.. The implication of the effect of solubility of ciprofloxacin on its absorption from the gut is highlighted. Experimental Equipment Thermostated shaker bath (Gallenkamp, UK) set at 37 ± 0.20C was used to shake the ciprofloxacin and ciprofloxacin metal cation solutions. Ultraviolet/Visible spectrophotometer (Ultrospec 3000, Pharmacia Biotech, Cambridge, UK) was used to take all the absorbance readings. Materials Pure ciprofloxacin hydrochloride monohydrate (Sam Pharmaceuticals, Nigeria) sulphuric acid (BDH Chemicals, UK), ferric ammonium citrate (May and Baker, India); ferrous sulphate heptahydrate, aluminium hydroxide, magnesium sulphate, calcium carbonate, and potassium chloride (Merck, Germany) and sodium bicarbonate (Halewood Chemicals, UK) were used as obtained. Method De-ionised water was used to prepare a stock solution of 0.05molL-1 sulphuric acid. This solution was used to prepare the solutions of ciprofloxacin and the metal cations. The solubility of ciprofloxacin alone was determined by weighing ciprofloxacin powder accurately into 5ml 0.05molL-1 sulphuric acid in a 20ml stoppered volumetric flask. This was then put in a thermostated shaker bath set at 37 ± 0.20C and shaken for five hours to attain equilibrium. An aliquot of the supernatant of the saturated solution was diluted serially with 0.05molL-1 sulphuric acid to produce a solution whose absorbance was measured at 277nm (wavelength of maximum absorption i.e. at λmax = 277nm). The concentration of ciprofloxacin corresponding to this final solution was interpolated from Beer’s plot of ciprofloxacin in 0.05molL-1 sulphuric acid previously prepared at 277nm. From the dilution factor, the original concentration of the saturated solution and hence the solubility of ciprofloxacin was calculated. The procedure was repeated in the presence of varying amounts of the different metal cations. Except for the determinations in the presence of magnesium sulphate where final absorbance readings were taken at 277nm, absorbance readings for the other determinations in the presence of other metal cations were taken between 360 and 370nm. Beer’s plot for ciprofloxacin in each ciprofloxacin-metal ion complex was made. This was done by taking varying weights of ciprofloxacin with the metal cation in 0.05molL-1 sulphuric acid and measuring their absorbances at the respective λmax between 360nm and 370nm. The concentration of ciprofloxacin in each ciprofloxacin – metal ion complex was interpolated from the Beer’s plot for the respective complex. Results and Discussion 0.05molL-1 sulphuric acid was used to mimic the acidity of the stomach. Some of the metal cations formed coloured solutions in 0.1molL-1 hydrochloric acid hence it was not used because it would significantly interfere with the spectral measurements. Shaking at 37 ± 0.20C for five hours was to mimic human gastrointestinal tract motility, body temperature and to attain equilibrium more readily. In the medium used here, Beer’s law was obeyed for ciprofloxacin at its λmax of 277nm. In the presence of metal cations studied (except for magnesium sulphate), ciprofloxacin formed complexes that absorbed radiation at longer wavelengths. Thus, to reduce the spectral interference of the metal cations, determinations in the presence of metal cations were made at longer wavelengths (between 360 and 370nm). In the presence of each metal cation, Beer’s law was obeyed for ciprofloxacin. The solubility of ciprofloxacin in the medium used here is 46.65mgml-1 (0.12M). This value shows that the drug has appreciable solubility at the pH of the stomach. Thus, with an adult dose of 250mg ciprofloxacin, dissolution of the drug would take place readily. Ross et al (25) have reported the solubility of 6.9 mgml-1 at 37oC for ciprofloxacin at a pH of 5. In the presence of drugs containing metal cations (except for magnesium sulphate), ciprofloxacin formed soluble complexes in acidic medium. The solubility of ciprofloxacin in the presence of varying amounts of metal cations are shown in Fig 1. In the presence of magnesium sulphate, there was no shift in the λmax of ciprofloxacin. This signified that no complex must have been formed. Sanchez et al (17) have reported a similar trend. They concluded that ciprofloxacin does not form co-ordination complex with polyvalent cations in acid medium. It was observed that in the presence of magnesium sulphate, the solubility of ciprofloxacin increased slightly from 46.65mgml-1 (0.12M) to 50mgml-1 (0.13M) as the amount of magnesium sulphate increased initially. Thereafter, the solubility of ciprofloxacin decreased progressively with increase in the amount of magnesium sulphate. At higher amounts of magnesium sulphate, there was precipitation. Ross et al (16) have also reported a similar decrease in the solubility of lomefloxacin (an analogue of ciprofloxacin) in acidic medium in the presence of Bi3+. They attributed this to formation of type B complex of Higuchi and Connors (26). A similar factor may be responsible for the observed trend here for ciprofloxacin in the presence of Mg2+. Moreover, Turel et al (24) have shown that ciprofloxacin forms an adduct with magnesium sulphate in which magnesium is not bonded to the quinolone molecule but rather, the magnesium ion is co-ordinated by six water molecules forming [Mg(H2O)6]2+ cation with a nearly regular octahedral geometry. They reported that it was the only example of a metal-quinolone ionic compound with the water molecules co-ordinated to the metal. The precipitation observed in this study may be of the magnesium adduct formed. The co-ordination of six water molecules to magnesium ion in aqueous solution of this adduct ties up water molecules. This will make less water molecules available to solubilize ciprofloxacin. Also, the lattice structure of this adduct is different from that of the other co-ordination complexes of ciprofloxacin (18) hence the different behaviour in its aqueous solubility. In the presence of the metal cations where there was a shift in the λmax of ciprofloxacin to longer wavelengths thus indicating metal cation co-ordination to ciprofloxacin, the complexes formed (hence the amount of ciprofloxacin in them) were progressively more soluble as the amount of metal cations increased. However, the extent of increase in solubility of ciprofloxacin was different in the presence of different metal cations. Ferrous sulphate caused the greatest increase in solubility of ciprofloxacin at all levels of the amount of metal cations. This was followed by ferric ammonium citrate, calcium carbonate and aluminium hydroxide. Potassium chloride and sodium bicarbonate caused similar but very little increases in the solubility of ciprofloxacin in acidic medium. Thus, the divalent and trivalent cations caused greater increases in the aqueous solubility of ciprofloxacin while the monovalent cations caused very slight increases. The increase in solubility of ciprofloxacin in the presence of these metal cations may be due to the formation of ionic and hydrated complexes which are more hydrophilic than ciprofloxacin. Ciprofloxacin has been reported to form metal cation complexes which have varying numbers of water of hydration (18 - 23). When a drug is administered as a tablet, the tablet will first disintegrate in the stomach and be dissolved before it is absorbed. To penetrate the gastrointestinal membranes of the stomach, the drug must possess appreciable lipophilicity (27). For a drug like ciprofloxacin that possesses a good dissolution and lipophilic properties and can thus penetrate the membranes of the stomach, any factor that enhances its hydrophilic properties will reduce its lipophilicity and thus decrease its penetration through the membranes of the stomach. This in turn will reduce the amount of the drug that will be absorbed and hence decrease bioavailability. The general implication of the increasing solubility of ciprofloxacin in the presence of the metal cations is the decrease in bioavailability under such conditions. However, from this study, different cations will elicit this effect to different extents. Ferrous sulphate will have a more profound effect while the monovalent cations will have less effect. The same decreased lipophilicity of ciprofloxacin in the presence of metal cations will account for the decreased antimicrobial activity of ciprofloxacin in the presence of metal cations as ciprofloxacin will be less able to penetrate the bacterial cell walls in such cases. From this study, the decrease in antimicrobial activity will vary to different extents in the presence of different metal cations and will be more as the amount of metal cations increase. Conclusion We propose that the reduced bio-availability of ciprofloxacin in the presence of metal cations is as a result of the formation of more ionic and water soluble complexes. This will make it to be less absorbable and also less antibacterially active. Ferrous sulphate, ferric ammonium citrate, calcium carbonate and aluminium hydroxide form water soluble complexes in acid medium with ciprofloxacin. This complexation will have profound effects on both the bioavailability and antibacterial activity of ciprofloxacin. It is therefore suggested that co-administration of ciprofloxacin with these metal cations be discouraged as this will compromise the therapeutic usefulness of ciprofloxacin. Sodium bicarbonate and potassium chloride showed little increase on the solubility of ciprofloxacin in acid medium and will have less adverse effects when co-administered with ciprofloxacin. Magnesium sulphate does not form any soluble complex with ciprofloxacin in acid medium. Thus, this in-vitro study predicts that in this medium, magnesium sulphate may not adversely affect the bioavailability and antibacterial activity of ciprofloxacin. However, because in-vivo conditions were not replicated completely, therapeutic observations may be different. References
Copyright @2002-2006. TJPR Faculty of Pharmacy, University of Benin, Benin City, Nigeria The following images related to this document are available:Photo images[pr05004f1.jpg] |
| |||||||||

{kind=link}